Download
1 / 21
210 likes | 341 Vues
State Strategies to Cover the Uninsured: The Public Sector. December 7, 2005 Charles Milligan, JD, MPH Adequate Health Care Task Force. Preview. State Coverage of the Uninsured: Medicaid State Coverage of the Uninsured: Pooling A Closing Thought on “Being Insured”.

E N D
State Strategies to Cover the Uninsured:The Public Sector December 7, 2005 Charles Milligan, JD, MPH Adequate Health Care Task Force
Preview • State Coverage of the Uninsured: Medicaid • State Coverage of the Uninsured: Pooling • A Closing Thought on “Being Insured”
Medicaid covers the uninsured in three ways. • Outreach: Enroll eligible but enrolled individuals (no policy change needed) • Expand eligibility to optional eligibility groups (no federal approval needed) • Use a “demonstration” (1115) waiver to cover an expansion group (federal approval needed)
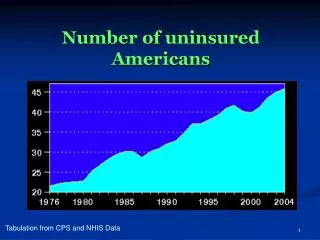
Outreach by itself may target the uninsured who are in the lower income categories . . .
In fact, most uninsured children already qualify for Medicaid or SCHIP.
Beyond outreach, states may expand eligibility to optional eligibility groups without a federal waiver . . . • Children up to 185% poverty (Medicaid) or 200% poverty (SCHIP) • Pregnant woman up to 185% poverty • Poor seniors to 100% poverty Yet a few states are cutting back, too, such as MO and TN
. . . or seek an 1115 federal waiver to cover expansion groups • Must be “budget neutral” • Thus, savings must be made in other parts of Medicaid to provide coverage • In 2001, CMS created a template for this, known as the “HIFA” waiver
. . . yet this growth reflected substitution as much as coverage of the previously uninsured . . .
One outcome of substitution is that pressure is increasing on Medicaid provider rates . . . State Medicaid Program Providers 1. Cannot cost shift onto Medicare or private insurance (due to “prudent purchasing” by these purchasers) 2. Increase in Medicaid enrollment/patient load heightens the importance of Medicaid rates 3.Providers: “social mission diluted by Medicaid expansions”
. . . and another is the so-called “Wal-Mart” bill in Maryland. • In the 2005 legislative session, Maryland’s legislature passed a bill on “pay or play” that singled out Wal-Mart. • Governor Ehrlich vetoed the bill.
These dynamics are leading to new thinking in Medicaid reform and coverage of the uninsured • Create disincentives for substitution of Medicaid for ESI • Mirror ESI movement to defined contribution (per capita cap) • Create “tiered” programs • Benefits • Cost sharing • Enrollment caps
1. Create disincentives for substitution of Medicaid for ESI • Premium assistance • Idaho, Illinois, Michigan • Mirror benefits and cost sharing • New Mexico, Oklahoma, Utah, Oregon, Tennessee Goals: link to private insurance to: • Shore up that market for employer purchasing • Shore up provider fees
2. Mirror ESI movement to defined contribution (per capita cap) • Defined contribution: Health Savings Account • South Carolina • Florida • Similarly, one goal is to shore up private insurer and provider markets • Another goal is to convert beneficiaries into prudent purchasers
Create “tiered” programs • Expansive benefits for mandatory Medicaid eligibles, limited benefits with cost sharing for others • Michigan • New Mexico • Iowa • Tennessee • Oregon
Other States Are Advancing “Pooling” Approaches to the Uninsured • Maine’s “Dirigo” Initiative • Connecticut’s “MEHIP” Initiative Yet, absent new finances, underlying economic challenges for coverage expansion remain
Questions Charles Milligan Executive Director, UMBC/CHPDM 410.455.6274 cmilligan@chpdm.umbc.edu www.chpdm.org