Download
1 / 28
310 likes | 1.33k Vues
Chest X-ray Findings in Heart Failure. Stefan Da Silva Jan 18 th 2007. Progression of findings Related to increasing pulmonary capillary pressures. Common Chest Xray Findings Increased Heart Size Cephalization of flow/Vascular Redistribution Interstitial Edema Pleural Effusions

E N D
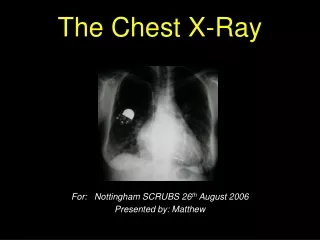
Chest X-ray Findings in Heart Failure Stefan Da Silva Jan 18th 2007
Progression of findings • Related to increasing pulmonary capillary pressures. • Common Chest Xray Findings • Increased Heart Size • Cephalization of flow/Vascular Redistribution • Interstitial Edema • Pleural Effusions • Aveolar Edema
Case #1 • 75 yr old male presenting with swelling in legs. • Vitals 37.6, 70 HR, 150/80, 18RR sats 94% RA
Increased Heart Size • Usually a cardiothoracic ratio of >0.50 • Sensitivity 54% - 79% (Knudsen et al., Fonseca et al) • Specificity 78% - 80% (Knudsen et al., Fonseca et al)
Dr. W. Roentgen • 1895 • 7 weeks of experiments after he discovered the “x” ray to produce the first image.
Case #2 • 75 yr old male with leg swelling and increasing SOB on exertion • Vitals 37.6, 70 HR, 150/80, RR 18 sats 94% RA
Vascular Redistribution • Usually lung bases better perfused than apices and vessels supplying lower lobes are larger than upper lobes. • Perivascular edema develops in lower lobes compresses vessels causes equalization of size of vessels between lower lobes and apices. • Upper vessel size > 3mm diameter
Vascular Redistribution con’t • Increasing pulmonary capillary pressure causes “cephalization of flow” due to shunting to upper lobe vessels. • Flip xray upside down • Poorly sensitive: 41% (as low as 17% in one study) • Specificity: 94 - 96% (Knudsen et al., Fonseca et al)
Case #3 • 75 yr old male with leg swelling and progressive SOB while at rest • Vitals 37.6, 90 HR, 170/90, RR 25 sats 89% RA
Interstitial Edema • (1) septal, producing Kerley lines (i.e., sharp, linear densities of interlobular interstitial edema); • (2) perivascular, producing loss of sharpness of the central and peripheral vessels; and • (3) subpleural, producing spindle-shaped accumulations of fluid between the lung and adjacent pleural surface.
Accumulation of fluid leads to • Indistinct hilar vessels • Kerley “B” lines (Kerley “A” lines: same significance but less common and seen more at inner lung fields towards hilum) • Fluid in the interlobar fissures • Peribronchial cuffing • Sensitivity: 17 - 27% (Knudsen et al., Fonseca et al) • Specificity: 95 - 98% (Knudsen et al., Fonseca et al)
Case #4 • 75 yr old male with leg swelling and increasing SOB at rest, diaphoretic. • Vitals 37.6, 100 HR, 180/96, RR 30 sats 85% RA
Pleural Effusions • Sensitivity: 1.2% - 25% (Knudsen et al., Fonseca et al) • Specificity: 92 - 99% (Knudsen et al., Fonseca et al) • Again seen with higher pulmonary capillary pressures ( > 25 mg Hg) • Commonly seen with patients with chronic heart failure
Case #5 • 75 yr old male with leg swelling, diaphoresis and marked SOB while at rest • Vitals 37.6, 110 HR, 190/100, RR >30 sats 78% RA
Alveolar Edema • Can lead to the “butterfly” or “batwing” appearance commonly described • Sensitivity 1.9% - 6% (Knudsen et al., Fonseca et al) • Specificity: 97 – 99% (Knudsen et al., Fonseca et al)
Take home points • 1 in 5 pts with acute decompensated heart failure with have no signs of congestion on chest xray (Collins et al.) • Poorly sensitive • Those with chronic heart failure may have subtle findings (Chakko et al.) • Beware of portable chest xrays