Recent
Recent. Anticoagulants. Introduction. Traditional anticoagulants in clinical use for the prevention or treatment of TED are heparin and its analogues and warfarin. They have two major limitations: a narrow therapeutic window and a highly variable dose-response relation.


Recent
E N D
Presentation Transcript
Recent Anticoagulants
Introduction • Traditional anticoagulants in clinical use for the prevention or treatment of TED are heparin and its analogues and warfarin. They have two major limitations: a narrow therapeutic window and a highly variable dose-response relation. • So, they require monitoring by laboratory testing.
Endothelium F VII TF TF/F VII F Xa F X TH PT Fibrinogen Fibrin
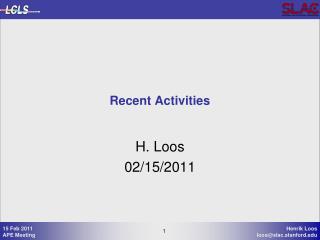
heparin and antithrombin Antithrombin (AT) neutralizes thrombin, factor Xa, and factor IXa, by forming irreversible complexes. Inhibition of thrombin and factor Xa by AT is relatively slow. However, binding of heparin to the heparin binding site on AT produces acceleration in the inactivating process by 1000-4000 fold by producing a change in the 3-D tertiary structure of AT .
Endothelium F VII TF TF/F VII AT F Xa F X TH PT Fibrinogen Fibrin
history Heparin first used in vascular surgery 1930’s Coumadin enters into clinical use 1950’s LMWH approved for use in US 1993
The Ideal Anticoagulant Bioavailable, predictable dose response High efficacy to safety index Administered parenteral or oral Rapid onset of action Available antidote Minimal interactions with other drugs
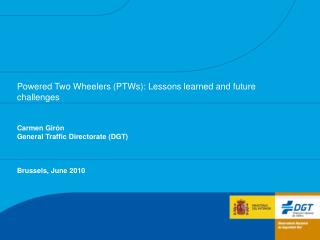
New Anticoagulants F VII TF Factor Xa Inhibitors Direct Indirect TF/F VII F Xa F X Thrombin Inhibitors Direct Indirect TH PT Fibrinogen Fibrin
Thrombin Inhibitors Hirudin Argatroban Bivalirudin Heparin LMWH Ximelagatran Dabigatran
Advantages of direct thrombin inhibitors over indirect inhibitors
Parentral DTI Argatroban It is a small molecule derived from L-Arginine, which interacts with the active site of thrombin. The Half life is 50 min and With 100% bioavailability. Dosing precautions are required in patients with hepatic dysfunction.
Parentral DTI Argatroban In 2000, it was licensed by the FDA for prophylaxis or treatment of thrombosis in patients with (HIT). In 2002, it was approved for use during PCI in patients who have HIT or are at risk for developing it.
Parentral DTI Argatroban Side Effects: Bleeding Hypotension Diarrhea Dyspnea Fever
Parentral DTI Argatroban • Pediatric use: • Open-label multicenter trial was conducted in pediatric patients (n=18 from 0-16y) • Estimated clearance of argatroban in pediatric patients was 2-fold lower than adults. • Body weight was significant predictor of argatroban clearance • Suggested that a starting dose of 0.75 µg/kg/min in pediatric patients was comparable in performance to 2.0 µg/kg/min approved in adults with aPTT follow. • Plasma concentration–aPTT relationship was used to derive a safe starting dose and titration scheme for the first time in pediatric patients and was incorporated into the US prescribing information for argatroban. Madabushi R, Cox DS, Hossain M, Boyle DA, Patel BR, Young G, et al. Pharmacokinetic and pharmacodynamic basis for effective argatroban dosing in pediatrics. J ClinPharmacol Jan;51(1):19-28.
Parentral DTI Lepirudin Is a recombinant hirudin approved for the treatment of (HIT). The half life is 1.3 hr and With 100% bioavailability. Caution should be used in patients with renal insufficiency since the drug is cleared by the kidney.
Parentral DTI Lepirudin About 40 -70 % of patients treated with lepirudin for more than five days develop anti-hirudin antibodies . These are not neutralizing antibodies and may actually enhance drug potency, perhaps by delaying its clearance from the circulation. Journal of the American Society of Hematology , October 1, 2000 vol. 96 no. 7 2373-2378 The aPTT needs to be monitored on a regular basis in such patients.
Parentral DTI Lepirudin Side Effects: Bleeding Allergic reaction High liver transaminases Worsening of heart failure
Parentral DTI Lepirudin Pediatric use: Appropriate studies have not been performed on the relationship of age to the effects of lepirudin in the pediatric population. Safety and efficacy have not been established. Although few reported case reports are saying it is effective in HIT.
Parentral DTI Bivalirudin Is a recombinant hirudin approved for the treatment of (HIT). The half life is 25 min and With unknown bioavailability. It undergoes predominant non-organ elimination (proteolysis).
Parentral DTI Bivalirudin Is frequently used for anticoagulation in the setting of invasive cardiology, particularly (PCI). Its affinity for thrombin is intermediate between that of lepirudin and argatroban.
Parentral DTI Bivalirudin Side Effects: Back pain is the most common side effect Hypotension Bleeding Urinary retention GIT upset
Parentral DTI Bivalirudin • Pediatric use: • The FDA granted pediatric exclusivity for bivalirudin, based on studies submitted in response to a written request by the FDA to investigate the use of bivalirudin in pediatric patients. • Study outcomes suggest that the (PK) and (PD) response of bivalirudin in the pediatric population is predictable and behaves in a manner similar to that in adult. • Forbes TJ, Hijazi ZM et al Division of Cardiology, 2011 Apr
Oral DTI Ximelagatran First oral direct thrombin inhibitor. Thought to be a substitute to warfarin Half-life 3-4 hours Eliminated by the kidneys Developed in 2004 and was withdrawn in 2006 due to hepatotoxicity
Oral DTI Dabigatran It offers an alternative to warfarin The Half life is 14-17 h with 6% Bioavailability . Renal excretion of unchanged drug is the elimination pathway.
Oral DTI Dabigatran The absorption is dependent on acidic medium. No drug or food interactions. Approved by FDA for Atrial fibrillation.
Oral DTI Dabigatran On March 18, 2008, EMA granted marketing of the drug for the prevention of TED following hip or knee replacement surgery and for non-valvular atrial fibrillation. On October 19, 2010 the FDA approved its use for prevention of stroke in patients with non-valvular atrial fibrillation
Oral DTI Dabigatran On February 14, 2011, The ACCF and AHA added it to their guidelines for management of non-valvular atrial fibrillation On December 7, 2011, the FDA initiated an investigation into serious bleeding events associated with dabigatran
Oral DTI Dabigatran Side Effects: Bleeding GIT upset Allergic reaction
Oral DTI Dabigatran Pediatric use: Appropriate studies have not been performed on the relationship of age to the effects of dabigatran in the pediatric population. Safety and efficacy have not been established.
Dabigatran Etexilate (DE) vs WarfarinPrevention of Stroke in Atrial Fibrillation • 18,113 pt. with A-fib, F/U 2 years • DE, 110 mg bid was non inferior to Warfarin in the primary end point • 150 mg bid was superior to Warfarin • The cumulative incidence of bleeding 0.38% Warfarin, 0.12% with DE • The incidence of dyspepsia was higher in DE leading to higher rate of discontinuation • ____________________ • Moia M et al N Eng J Med 2009, 361: 3672
Dabigatran Treatment of VTE: RECOVER-1 • Randomized trial, 2564 pts comparing • Dabigatran 150 mg bid vs Warfarin in the treatment of VTE for 6M after initial Rx with parenteral anticoagulant (9D) • Primary Efficacy: Non-Inferior • Safety: Lower rate of any bleeding: 16.1% vs 21.9% (P<0.001) • Major bleed: comparable • Death, ACS and LFTs: comparable
Factor Xa Inhibitors Rivaroxaban Apixaban Betrixaban Idraparinux
Indirect F Xa inhibitor Idraparinux Synthetic Pentasaccharidewhich is derived from fondaparinux. The half life is 80 h with 100% Bioavailability. once weekly Excreted unchanged in the urine, contraindicated in renal failure.
Indirect F Xa inhibitor Idraparinux Side Effects: Bleeding Renal impairment Allergic reaction
Indirect F Xa inhibitor Idraparinux Pediatric use: No available data about its use in pediatrics
Indirect F Xa inhibitor Idraparinux • Idraparinux versus standard therapy in the treatment of deep venous thrombosis in cancer patients: a subgroup analysis of the Van Gogh DVT trial. • Conclusion:In conclusion, no significant safety or survival differences were observed between cancer patients with DVT treated with idraparinux for six months compared to standard therapy. Fewer recurrent VTEs were observed in the idraparinux group; however, this was not statistically significant and also because of study limitations this should be interpreted with caution.. Thromb Haemost. 2010 Jul;104(1):86-91. Epub 2010 May 27
DirectF Xa inhibitor Rivaroxaban Oral direct Xa Inhibitor The Half life is 7-11 h, with 80-100 Bioavailability. 1/3 excreted unchanged by the kidney, 1/3 metabolized then excreted by the kidney, 1/3 metabolized by the liver and excreted in the bowel Inhibitors of CYP3A4 e.g. Ketoconazole and Ritonavir increase drug level in the circulation
DirectF Xa inhibitor Rivaroxaban Side Effects: Bleeding Allergic reaction Cholestasis Muscle spasm
DirectF Xa inhibitor Rivaroxaban Pediatric use: Appropriate studies have not been performed on the relationship of age to the effects of rivaroxaban in the pediatric population. Safety and efficacy have not been established.
Rivaroxaban in atrial fibrillation ROCKET-AF multisite, worldwide trial 14,000 pts at high risk of stroke randomized: Riv 20/15 mg/day vs warfarin Complex study population, high CHADs score: Riv non-inferior Risk of hemorrhagic stroke with Riv: 0.26% vs 0.44% Warfin Major bleeding similar: 3.6% vs 3.45% Cabral KP et al J Thromb Hemost 2011, 9:44
DirectF Xa inhibitor Apixaban Oral direct Xa Inhibitor The Half life is 8-14 h, with 50% Bioavailability. Multiple pathways of elimination: oxidative metabolism, renal (25%) and intestinal Advantage in pts with renal impairment
DirectF Xa inhibitor Apixaban A 2007 trial showed that apixaban was equivalent to enoxaparinopen-label study in preventing thrombosis in patients who had undergone a knee replacement. J Thromb Haemost. 2007 Dec;5(12):2368-75. Epub 2007 Sep 15. A 2010 trial showed that apixaban was superior to enoxaparin in preventing thrombosis in patients undergoing elective hip replacement surgery, with similar bleeding rates. N Engl J Med. 2010 Dec 23;363(26):2487-98.
DirectF Xa inhibitor Apixaban 2011 trial showed that in patients with A fib who have failed or are not candidates for warfarin, apixaban, as compared with aspirin, reduced the risk of stroke or systemic embolism in patients experiencing A fib by more than 50% The addition of apixaban, at a dose of 5 mg twice daily, to antiplatelet therapy in high-risk patients after ACS increased the number of major bleeding events without a significant reduction in recurrent ischemic events. N Engl J Med. 2011 Aug 25;365(8):699-708. Epub 2011 Jul 24.
DirectF Xa inhibitor Apixaban Pediatric use: The safety and efficacy of Apixaban in children below age 18 haven’t been established.
Apixaban in atrial fibrillation • Double blind randomized trail of 5599 pts with A-fib at increased risk of stroke for whom warfarin was unsuitable • Apixaban 5 mg bid vs ASA 81-325mg/day • Trial stopped: Apixaban clearly superior • Stroke or systemic embolism in 1.6% pts on Apixabanvs 3.47% ASA (P<0.001) • Major bleeding 1.4% vs 1.2% P=0.57 Conolly SJ et al N Eng J Med 2011, 364: 806
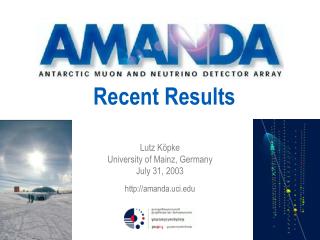
Suggested guidelines for the use of novel anticoagulants in children (medications in bold are first choice if applicable) American Society of Hematology , 2008
Refrences: UpToDate: 19.3 FDA.gov NewEnglandJournal PubMed MedScape Wikipedia