Download
1 / 63
790 likes | 1.27k Vues
Cancer Epidemiology In India. Ramesh Pawar Moderated by: Prof. Deshmukh Sir. Framework. Definition Introduction Magnitude Risk factors National programme Cancer registry and Atlas Cancer registry at MGIMS, Sevagram References . Cancer.

E N D
Cancer Epidemiology In India RameshPawar Moderated by: Prof. Deshmukh Sir
Framework • Definition • Introduction • Magnitude • Risk factors • National programme • Cancer registry and Atlas • Cancer registry at MGIMS, Sevagram • References
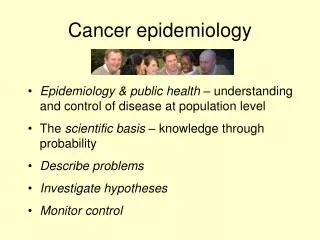
Cancer • Cancer refers to a class of diseases in which a cell or group of cells divide and replicate uncontrollably, intrude into adjacent cells and tissues( invasion) and ultimately spread to other parts of the body than the location at which they rose ( metastasis) ( national cancer Institute)
Introduction • India is experiencing a rapid health transition with rising burden of Non Communicable diseases (NCDs). • Overall NCDs are emerging as the leading cause of death and disability in India accounting for over 42% of all deaths (Registrar General of India). • According to national commission on macroeconomics and Health (NCMH) report (2005), the crude incidence rate for Cervix cancer, beast cancer and oral cancer is 21.3, 17.1 and 11.8 (among both men and women) per 100,000 population respectively. • Cancer registry data reveals that 48% of cancer in males and 20% in females are tobacco related and are totally avoidable. • 75-80% patients are in advanced stage of disease at the time of first attendance
Global Estimated age-standardised incidence and mortality rates: men and women WOMEN MEN Source: http://globocan.iarc.fr/factsheet.asp
Global Estimated age-standardised incidence and mortality rates: Men Source: http://globocan.iarc.fr/factsheet.asp
Global Estimated age-standardised incidence and mortality rates: Women Source: http://globocan.iarc.fr/factsheet.asp
Global Estimated age-standardised incidence and mortality rates: both men and women Source: http://globocan.iarc.fr/factsheet.asp
Men India: Estimated age-standardised incidence and mortality rates: men and women Women http://globocan.iarc.fr/factsheet.asp
India Estimated age-standardised incidence and mortality rates: Men http://globocan.iarc.fr/factsheet.asp
India Estimated age-standardised incidence and mortality rates: Women http://globocan.iarc.fr/factsheet.asp
Cancer Burden: India • Caner has become one of the ten leading causes of death in India. • It is estimated that there are nearly 2-2.5 million cancer cases at any given point of time. • 8-9 lakh new cases and 4 lakh deaths occur annually due to cancer. • Cancer of oral cavity and lungs and in males and cervix and breast in females account for 50% of all cancer deaths in India • WHO has estimated that 91% of oral cancers in SEAR directly attributable to the use of tobacco and this is the leading cause of oral cavity and lung cancer in India. • By 2050, there will be 17 million new cases in the developing world (Farlay et al 2004)
Risk factors for cancers: • Genetic factors • Retinoblastoma (RB1) • Interaction of gene and environment • Mutation in some p53 codons are more prevalent in cancer of a particular organ.
Risk factors • Infection • approximately 20% of the cancers among men and women in developing countries is attributed for infectious agents as opposed to 9% in developed countries.(Pisanil 1997) • Hep B & C, HPV. • Tobacco • Responsible for about 40 to 50% of cancers in men and about 20% of cancers in women
(Percentage) NFHS-3, 2005-06
(Percentage) Alcohol use by women is rare. NFHS-3, 2005-06
Risk factors • Diet • In India dietary habits responsible for about 10-20% of cancers. • The changing dietary patterns particularly involving animal proteins. • Consumption of large amount of red chillies, food at very high temperatures and alcohol consumption are the main risk factors for stomach cancer in India • Tuibur –Mizorum Source: WHO (2003) RTS 916. Diet, Nutrition and prevention of chronic diseases.
Risk factors Pesticides Malwa region of Punjab- a cotton belt “Cancer train” ( sengupta N.A. train ride to cancer care. Times of India 2011) • Breast cancer: late age at 1st pregnancy, single child, late menopause, high fat diet. • Cancer cervix: early marriage, multiple sexual partner, multiple pregnancy ,poor sexual hygiene. • Education and socio-economic status. • Physical inactivity and life style
Life style factors and risk of developing cancer Source: WHO TRS 916. Diet, nutrition and prevention of chronic diseases.
Disease should be an important public health problem • Must have a latent asymptomatic stage • Adequate treatment should be available • The test should be safe and relatively in-expansive • Capable of rapid application • Should be accurate and reproducible • Test should be acceptable to people • The test should be reasonably inexpensive • Adequate follow up of the positives should be ensured Undesired harm due to screening should be avoided
Early warning signals • If someone notice following symptoms she/he should contact to health centre immediately: • A sore that doesn’t heal • Recent changes in wart or mole • Unusual bleeding/discharge/per vagina/rectum • Persistent cough or hoarseness of voice • Persistent change in bladder/bowel habits • Difficulty in swallowing • Painless lump or swallowing.
National programme for prevention and control of cancer, diabetes, cardiovascular diseases and stroke • Pilot programme was launched on 4th January 2008 in 7 states covering one district each • Objectives • Prevent and control common NCDs through behaviour and life style changes. • Provide early diagnosis and management of common NCDs • Built capacity at various levels of health care for prevention, diagnosis and treatment of NCDs. • Train human resource within the public health setup viz doctors, paramedics and nursing staff to cope with the increasing burden of NCDs • Establish and develop capacity for palliative and rehabilitative care.
India Map showing the states to implement NPCDCS • Operational guidelines. (NPCDCS).Director General of Health services Ministry of health and family welfare Government of India.
Strategies • Prevention through behaviour change • Early diagnosis • Treatment • Capacity building of human resource • Surveillance, monitoring and evaluation
1. Prevention through behaviour change • Creating general awareness • Promotion of healthy life style habits • The various approaches such as mass media, community education and interpersonal communication • Increase intake of healthy food • Increased physical activity through sports, exercise etc. • Avoidance of tobacco and alcohol • Stress management • Warning signs of cancer etc.
2.A Early diagnosis • Strategy for early diagnosis of chronic non communicable diseases will consist of opportunistic screening of person above the age of 30 yrs at the point of primary contact with any health care facility, be it the village, CHC, district hospital, tertiary care hospital. • Opportunistic screening will have in built component of mass awareness creation, self screening and trained health care providers. • Involves simple clinical examination comprising of relevant questions and easily conducted physical examination (such as h/o tobacco consumption and measurement of blood pressure etc.)
2.B Treatment • Screening, diagnosis and management (including diet counselling, lifestyle management ) and home based care will be the key functions. • One of the nurse-home visit for bedridden cases. • Supervise work of health worker and attend monthly clinic held in villages on a random basis. • Advice patient about care • Refer if required. 2.C Home based care 2.C Referral
3.Palliative care • Affirms life and dying as a natural process • Neither hastens nor postpones death • Active total care of patients and families by multi-professional team.
Packages of services to be made available at different levels under NPCDCS
Management structure: • National NCD Cell • NCD Cell will be responsible for overall planning, implementation, monitoring, and evaluation of different activities and achievement of physical and financial target planned under the programme.
Role and responsibilities of National NCD Cell is as under • Plan, Coordinate, and Monitor all the activities at National and State level. • Develop operational guidelines, Standard Operating Procedures (SOP), Training modules, Quality benchmarks, Monitoring and reporting systems and tools. • Monitoring and evaluation of the programme through HMIS, Review meetings, Field observations, surveillance, operational research and evaluation studies. • Prepare National Training Plan: Curriculum, Training resource centres, training modules and organize national level training programmes • Procurement of equipment and supplies for items to be provided as commodity assistance; • Release of funds and monitoring of expenditure
State NCD cell • The Cell shall function under the guidance of State programme Officer (SPO NCD) and will be supported by the identified officers/officials from the Directorate /Director General of Health Services. SPO (NCD) will be a State level health official identified by the State government. • 1. State Programme Officer • 2. Programme Assistant • 3. Finance cum Logistics Officer • 4. Data Entry Operators (2)
A. Health promotion: • Behaviour and life style changes • Sub centre level • Carried out by the front line health workers- ANM and (or) Male Health Worker. • Camp, interpersonal communication (IPC), posters, banners • Educate people at community/school/workplace settings. Increased intake of healthy foods Increased physical activity through sports, exercise, etc.; Avoidance of tobacco and alcohol; Stress management Warning signs of cancer etc.
B Opportunistic Screening • During the camps/ designated day ANM and (or) Male Health Worker also examine persons at and above the age of 30 years for alcohol and tobacco intake, physical activity, blood sugar and blood pressure. • During the examination, health worker shall also carry out the measurement of weight, height, and Body Mass Index (BMI) etc. • C. Referral • ANM and (or) Male Health Worker refer the suspected case of Diabetes and Hypertension to the CHC or higher Health Facility for further diagnosis and management • D. Data recording and reporting • ANM and (or) Male Health Worker at Sub Centre maintain in prescribed format to related CHC under the programme and submit the report monthly to CHC.
Activities at Community Health Centre • A. Screening • B. Prevention and health promotion • C. Laboratory investigations • D. Diagnosis and Management • E. Home based care • F. Referral • Human Resources for CHC NCD services a. Doctor (1) b. Nurses (2) c. Counsellor (1) d. Data Entry Operator (1)
Activities at District Level • The selected districts provide the full complement of preventive, supportive and curative services for NCD • ‘NCD clinic’ • A. Opportunistic screening • B. Detailed investigation • C. Outsourcing of certain laboratory investigations • D. Out-patient and In-patient Care • E. Day Care Chemotherapy Facility • F. Home Based Palliative Care • G. Referral & Transport facility to serious patients • H. Health promotion • I. Training • J. Data recording and reporting
K. Human Resources at District Hospital • a. Doctor (specialist in Diabetology/Cardiology/M.D Physician) • b. Medical Oncologist • c. Cyto-pathologist • d. Cytopathology Technician • e. Nurses (4): 2 for Day Care, one for Cardiac Care Unit, one for O.P.D • f. Physiotherapist • g. Counsellor • h. Data Entry Operator • i. Care coordinator
National cancer registry Programme: • Cancer registration is the process of systemically and continuously collecting information on malignant neoplasm. • National cancer registry programme was launched in 1982 by ICMR to provide true information on cancer prevalence and incidence • Objectives: • To generate authentic data on the magnitude of cancer problem in India • To undertake epidemiological investigations and advice control measures and • Promote human resource development in cancer epidemiology.
National cancer registry Programme: • Population based cancer registries: there are 23 PBCR. Initially 5 in urban areas ( Delhi, Bhopal, Mumbai, Bangalore, Chennai ) and one in rural area ( Barshi In Maharashtra) • Hospital Based Cancer registries: at Chandigarh, Dibrugarh, Thiruvananthapuram, Bangalore, Mumbai and Chennai, six hospital based registries are maintained. • A total of 3.3% population is covered by these registries (12.8% Urban and 0.06% rural population).
National cancer registry Programme: • These registries generate annual report • From these registries, trends are indicating to put more emphasis on cancer prevention.