Download
1 / 80
800 likes | 1.02k Vues
Learn about the congenital anomaly of phimosis and painful paraphimosis. Understand the causes, symptoms, pathophysiology, risks, complications, and treatment options, including medical and surgical interventions.

E N D
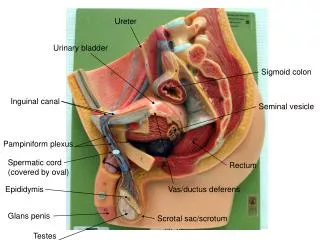
SURGERY OF THE PENIS AND URETHRA
Congenital Anomaly : • Agenesis Penis • Micropenis/Microphallus • Buried Penis (Concealed/Hidden/Trapped) • Phimosis • Paraphimosis • Hypospadias • Epispadias
Infection of the penis : balanopostitis Penile Cancer Urethritis Urethral Stone Urethral Strictures
Phimosis Description • inability to retract the foreskin • phimosis at the first few years is physiologic • the foreskin cannot be retracted after it has previously been retractable pathologic phimosis • by age 3.5 years, most foreskins can be retracted
Epidemiology • 10 % of boys have non retractile foreskin • 1 % at puberty Signs and symptoms • discharge, soiling of undergarment • irritation, cracking, bleeding from foreskin Pathophysiology Physiologic phimosis • the glans penis is adherent to the prepuce in infants • glandular secretions and smegma facilitate separation
Pathologic phimosis • cicatricialpreputial ring (from irritation result in inflammation and scarring) : poor local hygiene, chronic balanitis (Diabetes Mellitus), early forceful retraction of foreskin • balloon during voiding
Risk factors / causes Pathologic phymosis • poor hygiene, chronic balanopostitis, diabetes mellitus Complications • infection, increased risk of penile cancer
Defferential Diagnosis • physiologic phimosis • pathologic phimosis • post circumcision phimosis
History • hygiene problems ? • history of balanopostitis ? • history of diabetes mellitus ? • ballooning of foreskin when voiding ? • post – void dribbling ? • has there been a prior circumcision ? • could the foreskin be previously retracted ?
Physical Examination • Classification of retractability of the foreskin 0 : full retraction 1 : full retraction, tight behind glans 2 : partial exposure of the glans 3 : partial retractil, meatus just visible 4 : slight retraction, unable to visualize meatus 5 : no retraction
frenular lacerations • preputial fissure • cicatricial band • inflammation or active infection • “foreskins pearl” / smegma collection • evidens of malignancy
Laboratory testing • serum glucose to evaluate for diabetes • culture and sensitivity of the subpreputial space Imaging : none Special studies : none
Physiologic phimosis • encourage good hygiene • gentle cleaning of smegma • instruct parents in gentle and gradual retraction of prepuce • never circumcise in patient with hipospadias, prepuce may needed for reconstruction
Pathologic phimosis • good hygiene • steroid ointment • infection ------ antibiotics systemic or topical
Treatment Medical • local steroid application ( topical vs injection ) • nonsteroidal drug application ( cream ) Surgical Phisiologic phimosis • circumcision ( not absolutely indicated ) • surgical correction of phimosis with preservation of the foreskin
Pathologic phimosis • circumcision ---- standard of care • preputial dilatation • dorsal / ventral slit • surgical correction with preservation of foreskin
Alternative therapies : none Patient education : none Monitoring post circumcision • Post circumcision phimosis • inadequate primary procedure, post procedure scarring • may occure with Gomco clamp, Guillotin techniques • requires surgical revision • glandular hyperaesthesias ( take several month after circumcision / epithelium develops squameus keratinized layer
Complication of circumcision • is low ( 0,2 % - 0,6 % ) • hemorrhage • infection • avascular necrosis • meatal stenosis • fibrous bridge
urethrocutaneus fistula • concealed penis • penile denudation • lymphedema penile • Prevention : none • Associated condition : diabetes mellitus
Paraphimosis Discription Painful swelling of the foreskin distal to a phimotic ring after retraction of the foreskin for a prolonged period.
Pathophysiology In children • A congenital narrowed preputial opening is present • The foreskin is retracted behind the glans penis and not promptly reduced • Entrapment in the coronal sulcus occurs secondary to swelling of the glans • This lead to venous congestion, edema, and enlargement of the glans, • followed by arterial occlusion and necrosis of the glans
In adults • Typically occurs in elderly men and may be associated with poor hygiene and/or chronic balanoposthitis • This iflamation leads to a contraction of the opening prepuce and forms a fibrotic ring of tissue
This in turn leads to constriction when the foreskin is retracted behind the glans • Result in venous congestion with edema • Failure to promptly reduce the paraphimosis can result in arterial occlusion and necrosis of the glans penis. This constitutes a urologic emergency
Cause/risk factor • Phimosis • Chronic balanoposthitis • Chronic indwelling Foley catheterization and catheter changes • Patients requiring clean intermittent catheterization Complication • Necrosis of glans and distal urethra
Differential diagnosis • Balanitis • Balanoposthitis • Angioneurotic edema • Anasarca edema
Hystory • Has the patient been circumcised ? • Recurrent bouts of chronic balanitis ? • Chronic indwelling Foley catheterization ? • Clean intermittent catheterization ? • Diabetes mellitus : may be risk factor for phimosis • Phimosis ?
Physical examination • Edema and swelling of penile shaft proximal to the glans and corona • Thick phimotic ring proximal to corona • Late finding : swelling of the glans, venous congestion, necrosis of the glans penis.
Laboratory Testing • Not usually necessary • If surgery planned, preoperative laboratory studies, including coagulation factors Imaging: Chest film, if surgery planned General Measures • Considered urologic emergency • Delay in reducing paraphimosis can result necrosis of the glans
Medical • Gentle steady pressure to foreskin to decrease swelling (May use elastic wrap or Kerlix bandage) • Push the glans with thumbs, pulling the foreskin forward over the glans with the fingers ( Use the gauze pad to facilitate traction on the foreskin )
As an adjunct to simple reduction, a 25 – gauge needle is used to make multiple stab wounds in the edematous foreskin to help remove edema fluid May use 2 % lidocaine gel for local anesthetic • Hyaluronidase 1 cc ( 150 U/cc Wydase ) injected into the one or more sites in the edematous prepuce
Surgical • Dorsal or ventral slit using 1 % lidocaine penile block • Convert to normal circumcision
Follow – Up • Circumcision should be performed when the edema/inflammation resolves • If there is no definitive treatment, paraphimosis tends to recur • Debridement of necrotic tissue is rarely indicated
Prevention When inserting or changing Foley catheters or performing clean intermittent catheterization, reduce the foreskin after the procedure is completed
Hypospadias Description • Common urogenital malformation in males, characterized by incompletely formed urethra wherein the misplaces meatus variably opens on the ventral aspect of the penis, scrotum, or perineum.
Malformation varies greatly in severity, ranging from the extreme form of perineal hypospadias with genital ambiguity to mild distal glans hypospadias. Commonly associated with chorde (abnormal curvature of the penis) in 50 % of the cases and/or meatal stenosis 30 % of cases.
Epidemiology • Incidence 1 in 300 live male births • More common in Whites than in Blacks, and in Italians and Jews than in other ethnic groups Genetics • Familial tendency 8 % of fathers of affected children have hypospadias, • 14 % of male siblings affected
Staging Classification • Based on location of meatus : glans, subcoronal, penile, penoscrotal, scrotal, perineal • Distal hypospadias (subcoronal or penile) comprises 60 % of cases
Sign and Symptoms Associated anomalies • Undescended testicle: 9 % • Inguinal hernias: 9 % • Clinically significant upper tract anomalies ; rare Chordee • Chordee can occur without hypospadias, but is rare ( 0,6 % )
Pathophysiology • Unknown, but several factors involves • Alterations of urethral fold closure result in hypospadias • Testosterone biosynthetic defects occur in half proximal hypospadias
Exposure to synthetic “ endocrine disrupters” that block the effect of testosterone is critical from 9 to 12 weeks gestation • Related to low birth rate in discordant monozygotic twins
Cause/Risk Factors • Unknown, some suggestion of familial risk Complications • Infertility • Psychological trauma ( Cosmetic )
Differential Diagnosis • Glandular • Subcoronal • Penile • Penoscrotal • Scrotal • Perineal
History : any family history ? Physical Examination • The urethral opening may be anywhere along the shaft of the penis or into the perineum, 62 % of the openings subcoronal or penile, 22 % penoscrotal angle, and 16 % scrotum or perineum • Severe proximal hypospadias may be confused with intersex disorders • The more proximal meatus, the more the ventral curvature (chordee) will be seen • Undescended testes and inguinal hernia
Laboratory testing • If surgery planned Imaging • Incidens of upper urinary tract abnormalities is rare. With more severe ( proximal ) cases of hypospadias, some recommended screening the upper tract
Treatment General measures • With any suspicion hypospadias, neonatal circumcision should not be perfomed • Many consider severe hypospadias to be a type of intersex disorder
Surgery Treatment of the hypospadias is surgical repair and the timing of repair is best • between 6 and 18 months • Current techniques are superior than the older techniques • Short – term follow – up examinations for development of fistulas/stricture Alternative therapies is psychosocial support as part of overall care