Download
1 / 74
770 likes | 1.12k Vues
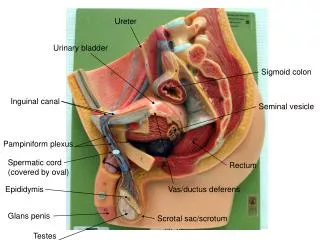
Surgery of the Penis and Urethra Ch.Reading. By: Dr. Ali AL- Amiri R2 Academic Day. PRINCIPLES OF RECONSTRUCTIVE SURGERY. The term tissue transfer implies the movement of tissue for purposes of reconstruction All tissue has physical characteristics: extensibility inherent tension

E N D
Surgery of the Penis and UrethraCh.Reading By: Dr. Ali AL-Amiri R2 Academic Day
PRINCIPLES OFRECONSTRUCTIVE SURGERY • The term tissue transfer implies the movement of tissue for purposes of reconstruction • All tissue has physical characteristics: • extensibility • inherent tension • viscoelastic properties of stress relaxation and creep. • physical characteristics of a transferred unit are primarily a function of the helical arrangement of collagen along with the elastincrosslinkages
PRINCIPLES OFRECONSTRUCTIVE SURGERY • Type of tissue transfer: A – Graft : that tissue has been excised and transferred to a graft host bed , where a new blood supply develops by a process termed take • Take requires approximately 96 hours and occurs in two phases • The initial phase, imbibition, requires about 48 hours • second phase, inosculation, also requires about 48 hours and is the phase in which true microcirculation is reestablished
Graft • Split-thickness : • carries the epidermis and also exposes the superficial dermal (intradermal or intralaminar) plexus • physical characteristics are not carried, which accounts for the tendency of split-thickness units to be brittle and less durable • favorable vascular characteristics • Full-thickness : • Carries superficial dermis and deep dermis or deep lamina • Carries characteristics attributable to that layer • fastidious vascular characteristics • does not contract
Graft • The grafts that have been successfully used for primary urethral reconstruction are the full-thickness • skin graft • bladder epithelial graft ( good vascular characteristics) • oral mucosal graft (optimal vascular characteristics) • rectal mucosal graft
Flap • Flap: implies that the tissue is excised and transferred with the blood supply either preserved or surgically reestablished at the recipient site Classification • vascularity ( random vs axial ) • Random : without a defined cuticular vascular territory • Axial : defined vessel in the base of the flap • Peninsula:vascular continuity and the cutaneous continuity of flap base are intact • Island: The vascular pedicle is intact; the cuticular continuity has been divided. • Microvascular free-transfer:The free-flap cuticular and vascular connections are interrupted at the base of the flap
Generalities of ReconstructiveSurgical Techniques • Reconstructive surgery is performed with all efforts aimed at minimizing tissue injury and promoting healing • Adequate visualization, Surgical loupes , headlight • In penile cases such as reconstruction of the fossanavicularisbipolarcautery is used exclusively • Sharp scissors that cut with minimal collateral trauma are essential • choice of suture • urethral surgery, absorbable suture is the rule • flap or graft repair, 4-0 to 6-0 suture is usually adequate
Reiter Syndrome • classic triad of arthritis, conjunctivitis, and urethritis • Urethral involvement is usually mild, self-limited, and a minor portion of the disease • 10% - 20% of patients have a calledcircinatebalanitis, is diagnostic of Reiter syndrome • shallow, painless ulcer with gray borders • mild and self-limited, no treatment is necessary • In severe cases: perinealurethrostomy and excise the entire distal urethra may be performed
Lichen Sclerosus (BalanitisXeroticaObliterans) • chronic inflammatory disorder of the skin of uknown origin • The peak ages • women are bimodal (before puberty and postmenopausal) • 30 to 50 years ( all ages ) • most common cause of meatalstenosis • LS appears as a whitish plaque that may involve the prepuce, glans penis, urethral meatus, and fossanavicularis • If only the foreskin is involved, circumcision may be curative • Diagnosis is made through biopsy
Lichen Sclerosus (BalanitisXeroticaObliterans) • cause of LS has not been defined , but suggested to be an autoimmune disease Treatment : • combination of topical steroids and antibiotics may help stabilize the inflammatory process • Conservative therapy may be warranted in patients whose meatus can easily be maintained at 14 F • intermittent catheterization with lubrication of the catheter and meatal dilator may be adequate treatment
Lichen Sclerosus (BalanitisXeroticaObliterans) • In young patients with severe meatalstenosis, surgery is indicated • Because LS is a disease of genital skin, better tissue for reconstruction is the oral mucosa • In severe urethral stricture disease • completely reconstructed the urethra • simply performed a perinealurethrostomy
UrethrocutaneousFistula • Urethral fistulas may be a complication of • urethral surgery • secondary to periurethral infection associated with inflammatory strictures • Treatment of a urethral fistula must be directed defect the underlying process • After urethral surgery • early fistula is the result of poor local healing, possibly secondary to hematoma, infection, or tension with closure • aggressive local care and continued urinary diversion may close fistula
UrethrocutaneousFistula Closure of fistula after surgery: • If small : • button of skin is removed from around the fistula • edges are cut flush with the urethral wall. • The urethra is closed with small (6-0 or 7-0) absorbable suture • If large : • local flaps will be required.
UrethrocutaneousFistula • Fistulas associated with inflammatory strictures develop secondary to high-pressure voiding of infected urine • multiple tracts develop called (watering pot perineum) • Repair requires • suprapubic drainage • treatment of the infection requires incision and drainage of any abscesses • We widely excise the fistula tracts • Flap reconstruction can be used • wait 4 to 6 months before repairing the underlying stricture • fistula or periurethral abscess may be the hallmark symptom of urethral carcinoma
Paraphimosis, Balanitis, and Phimosis • Paraphimosis: painful swelling of the foreskin distal to a phimotic ring, occurs if the foreskin remains retracted for a prolonged time • gentle steady pressure must be applied to the foreskin to decrease the swelling • If it reduced : elective dorsal slit or circumcision later • If failed emergency dorsal slit or circumcision • Balanitis: inflammation of the glans, can occur as a result of poor hygiene, from failure to retract and clean under the foreskin • Tx : local care and antibiotic ointment • Phimosis: inability to retract the foreskin, can result from repeated episodes of balanitis • Tx : circumcision
Urethral MeatalStenosis • Meatalstenosis in a boy appears to be a consequence of circumcision • Meatalstenosis occurs in adults after inflammation, specific or nonspecific urethral infection, and trauma • Tx • ventral urethral meatotomy • necessary to place sutures to approximate the urethral mucosal edge to control bleeding. • three sutures: one at the apex and one on either side
Circumcision • It is important not to circumcise any boy with a penile abnormality (e.g., hypospadias, chordee) that may require the foreskin during repair. • Indication for circumcision in the young boy • recurrent UTI thought to be associated with the redundant preputial skin • Monopolarelectrocautery should be avoided in a neonatal circumcision
URETHRAL STRICTURE DISEASE • urethral stricture: refers to anterior urethral disease, or a scarring process involving the spongy erectile tissue of the corpus spongiosum (spongiofibrosis) • Contraction of this scar reduces the urethral lumen • posterior urethral “strictures” are not included in the common definition of urethral stricture • obliterative process has resulted in fibrosis and is generally the effect of distraction in that area caused by either trauma or radical prostatectomy • By consensus of the WHO conference, the term stricture is limited to the anterior urethra.
The anatomy of anterior urethral strictures includes, in most cases, underlying spongiofibrosis. A, Mucosal fold. B, Iris constriction. C, Full-thickness involvement with minimal fibrosis in the spongy tissue. D, Full-thickness spongiofibrosis. E, Inflammation and fibrosis involving tissues outside the corpus spongiosum. F, Complex stricture complicated by a fistula.
Etiology • Any process that injures the urethral epithelium or the underlying corpus spongiosumto the point that healing results in a scar can cause an anterior urethral stricture • Trauma ( straddle trauma - iatrogenic ) • inflammatory strictures ( gonorrhea –BXO ) • Congenital if it is • not an inflammatory stricture • short-length stricture • not associated with a history of or potential for urethral trauma • Mainly limited to infants before they attempt erect ambulation
Diagnosis and Evaluation • Patients often present with • obstructive voiding symptoms • UTI (prostatitis , epididymitis) • urinary retention. • For an appropriate treatment plan you should know : • Location • Length • Depth • Density of the stricture (spongiofibrosis)
The length and location • determined with radiography, urethroscopy, and ultrasonography. • The depth and density • determined by P/E • appearance of the urethra in contrast-enhanced studies • the amount of elasticity noted on urethroscopy • The depth and density of fibrosis are difficult to determine objectively
Dynamic radiographic studies : • retrograde injection of contrast material and while the patient is voiding • If the patient is not in steep lateral oblique position for retrograde urethrography, the length of the stricture will be underestimated • evaluate the urethra proximal and distal to the stricture with endoscopy during surgery to ensure that all the involved urethra is included in the reconstruction
Treatment Dilation • oldest and simplest treatment • epithelial stricture without spongiofibrosis, it may be curative • goal is to stretch the scar without producing more scarring • least traumatic method is to use soft techniques over multiple treatment sessions. • Safest is balloon-dilating catheters
Internal Urethrotomy • refers to any procedure that opens the stricture by incising it transurethrally • incision through the scar to healthy tissue • to allow the scar to expand and the lumen to heal enlarged • Usually done by single incision at the 12-o’clock position • cross section of the corpus spongiosum, showed the thinnest portion of the anterior aspect is from 10-o’clock to 2-o’clock
Internal Urethrotomy • Complications: • recurrence of stricture ( most common ) • Bleeding • extravasation of irrigation fluid into the perispongiosal tissues • creation of a fistula (corpus spongiosum and the corpora cavernosa) • The data show that strictures at the bulbous urethra that are less than 1.5 cm and not associated with dense, deep spongiofibrosis • 74% moderately long-term success rate • F.cath to be kept for 3 to 7 days
Internal Urethrotomy • Urethral stents (removable or permanently implantable) after internal urethrotomy - UroLume( permanent ) • 6 months to 1 year • Available data show that the stent is best employed for relatively short strictures of the bulbous urethra associated with minimal spongiofibrosis • Complications: • perineal pain • Migration
Internal Urethrotomy Lasers • The ideal laser for urethral stricture disease • totally vaporizes tissue • exhibits negligible peripheral tissue destruction • not absorbed by water • easily propagated along a fiber • Advocates of the use of a contact laser suggest that it obliterates the scar by vaporization ( YAG) • results with use of these fibers are no better than those with direct cold-knife visual internal urethrotomy
Open Reconstruction Excision and Reanastomosis • complete excision of the area of fibrosis, with a primary reanastomosis of the normal ends of the anterior urethra • Most IMP technical points: • area of fibrosis is totally excised • anastomosis is widely spatulated, • large ovoid anastomosis • anastomosis is tension free. • Strictures of 1 to 2 cm are generally easily excised with reanastomosis
Four grafts that have been successfully used for primary urethral reconstruction are the • full-thickness skin • the bladder epithelial • oral mucosal (buccal, labial, lingual) • rectal mucosal • Grafts have been most successfully employed in the area of the bulbous urethra
Flaps • A number of applications of genital skin islands, mobilized on either the dartos fascia of the penis or the tunica dartos of the scrotum, have been proposed for the repair of urethral stricture disease • important considerations for the use of flaps: • nature of the flap tissue • vasculature of the flap • mechanics of flap transfer • For donor site consideration, it is most convenient to use the areas of redundant nonhirsute genital skin
in a meta-analysis of graft onlay procedures compared with flap procedures, showed equivalent results for graft operations and flap procedures.
PELVIC FRACTURE URETHRAL INJURIES • Urethral injuries accompany about 10% of pelvic fracture injuries • Distraction injuries are for all intents unique to the membranous urethra • Many injuries appear not to totally distract the entire circumference of the urethra • placement of an aligning catheter may allow the urethra to heal virtually unscarred or with an easily managed stenosis
Repair • It is desirable to proceed within 4 to 6 months after trauma • The classic reconstruction consists of a spatulatedanastomosis of the proximal anterior urethra to the apical prostatic urethra • Several series support the concept that the bulk of pelvic fracture urethral injuries can be managed by the perineal approach • At the time of reconstruction • endoscopy is performed through the meatus and again through the suprapubic tube sinus • To R/O vesicolithiasis