Role of Imaging in HIV: CNS Pathologies and CD4 Count Correlation
690 likes | 789 Vues
Understand the critical role of imaging in managing HIV patients with CNS involvement, correlating pathologies with CD4 counts, and diagnosing a wide range of conditions including encephalitis, lymphoma, and opportunistic infections.

Role of Imaging in HIV: CNS Pathologies and CD4 Count Correlation
E N D
Presentation Transcript
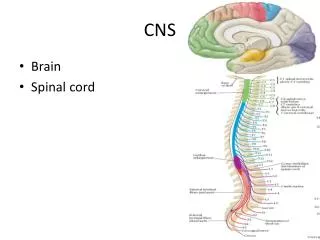
CNS involvement in HIV DR. ASHISH CHINDHALORE, JRIII GUIDE - DR. POOJA DESHPANDE, ASST. LECTURER
ROLE OF IMAGING Imaging plays important role in the management of HIV. 1. In view of overlap of clinical symptoms, imaging helps to identify the pathology in correlation with clinical symptoms & CD4 count. 2. It plays important role in identifying acute pathologies like cerebral infarcts, PCP pneumothorax, TB /Toxoplasma involvement, HIV Encephalopathy v/s PML 3. Imaging helps to study changing trends in HIV ,in view of early antiretroviral therapy.
CD4 COUNT AND PATHOLOGIES CD4 COUNT PATHOLOGY 600-800 Asymptomatic 400-600 Tuberculosis <400 Oral candidiasis Cryptosporidiosis Lymphoma <200 Kaposi`s sarcoma HSV,CMV(<50-100) PCP MAC Toxoplasma, PML , HIV - Encephalopathy Cryptococcal meningitis (<50-100). Esophageal candidiasis
Diseases occurring in brain in HIV patient: 1.Primary effects of HIV: • AIDS Dementia complex • HIV encephalopathy. 2.Opportunistic infection: • Progressive multifocal leukoencephalopathy CMV encephalitis Herpes encephalitis • Toxoplasmosis • Cryptococcosis • Neurosyphilis • Bacterial and fungal abscesses • Meningitis- Tubercular -Cryptococcal • Ventriculitis 3.Neoplasm • Primary CNS lymphoma • Gliomas • Kaposi’s sarcoma 4.Vasculitis 5.Immune reconstitution inflammatory syndrome.
HIV ENCEPHALITIS • Direct result of HIV brain infection. • ETIOLOGY- HIV-1 • Clinical issues- HANDs m/c clinical manifestation. 60% of patients devlop neurologic disease. 15-25% of treated patients devlop AIDS dementia complex. • Pathology - • Gross - Early stage brain grossly normal and GCA in late stage.
HIV ENCEPHALITIS • NECT- Normal or atrophy +/- WM hypodensity. • MR- • Volume loss with prominent sulci and ventricle. • T2/FLAIR hazy symmetric WM hyperintensity, spare the subcortical U fibers. • No mass effect. • Usually no enhancement and no restricted diffusion. • T1 images reveal no hypointensity. • Reduced grey matter volume in superior and medial frontal gyri – possible early imaging marker. D/D- PML, CMV enchephalitis, ventriculitis; toxoplasmosis; Herpes and HHV-6 encephalitis.
Progressive Multifocal Leukoencephalopathy • ETIOLOGY- JC virus. Ubiquitous virus. • Immunodificiency. Most common predisposing condition = HIV (80%). • Three phases of devlopment. • Virus exclusively affect the oligodendrocytes. • Multifocal demyelination. • Predominantly affect parietal & occipital lobes. posterior fossa white matter and basal ganglia involvement is also present. • CNS manifestation are cPML ,iPML, JC encephalitis/meningitis.
IMAGING: Multifocal WM lesions but may be unifocal. Bilaterally assymetric. Involve subcortical U fibers. Spare cortex. No mass effect/enhancement (except iPML) On DWI, varies according to disease stage. MRS- Decrease NAA, increased choline and lipid lactate peak. pMRI – shows reduced rCBV. D/D- HIVE, PML-IRIS, CMV.
Tuberculosis • Most common infection in Indian setting. • Etiology: Reactivation of prior infection Rapid dissemination of newly acquired infection. • Causative agent- M. Tuberculosis.
Imaging features: Radiological findings seen in CNS TB are • Cisternal/meningeal enhancement. • Hydrocephalus. • Enhancing parenchymal lesions. • Tubercular abcess. • Vasculitis/Infarcts.
Cisternal/meningeal enhancement • Commonly involved sites are the interpeduncular cistern, pontine cistern, perimesencepalic and suprasellar cisterns. • The sulci over convexities, sylvian fissures and tentorium can also show enhancement.
Hydrocephalus • Communicating type: obstruction of basal cisterns by inflammatory exudates. • Non communicating type: Due to parenchymal lesion causing mass effect or due to the entrapment of a part of ventricle by granulomatous ependymitis.
Enhancing parenchymal lesions(Tuberculoma) • Tuberculomas can be single or multiple and present anywhere in brain parenchyma. • Usually conglomerated and coalesce to form non caseating granuloma, which further in most cases show central caseous necrosis and eventually liquefaction.
Depending on its stage of maturation tuberculoma’s appearance varies on MRI. • Stages of tuberculoma: Non caseating Caseating with solid centre Caseating with liquid centre
Non caseating • Hyperintense onT2W images and slightly hypointense on T1W images with homogeneous post contrast enhancement.
Caseating with solid centre: • Hypo to isointense on both T1W and T2W images with an iso to hyperintense rim on T2W images. • In presence of an edema rim is inseparable on T2W images. • Shows rim enhancement on post contrast T1W images.
Caseating with liquid centre: • When the solid centre liquefies it appears hyperintense on T2W images with surrounding hypointensity. • On post contrast images show rim enhancement.
Differential diagnosis of tuberculoma • Healing stage of neurocysticercosis. • Fungal granulomas. • Pyogenic abscesses and lymphoma.
Tubercular abcess • Large multiloculated ring enhancing lesions with surrounding edema and mass effect on MRI. • DWI shows restricted diffusion with low apparent diffusion coefficient (ADC).
DIFFERENTIAL DIAGNOSIS Tubercular abcess Pyogenic abcess • MTR values in the rim of tubercular abscesses (19.89+/-1.55) due to high lipid. • MRS-Only lactate and lipid peaks (0.9 and 1.3 ppm) in tuberculous abscesses. • MTR-(24.81 +/- 0.03). • MRS-Cytosolic amino acid peaks (val, isoleucine, leucine) are seen.
Tubercular Vasculitis/Infarcts • Vascular occlusion is common sequel of tubercular arteritis. • MCA and leniticulostriate arteries are most commonly involved. • Majority of infarcts are in basal ganglia and internal capsule region. • Diffusion weighted imaging helps in early detection of infarcts.
Toxoplasmosis • Infection by parasite T. gondii, present as altered sensorium, headache and mild hemiparesis. • Multifocal involvement more common than solitary. • Typically Supra-tentorial. • Corticomedullary junction , Basal Ganglia, Thalamus, Intraventicular. • Necrotising abscess. • D/D-Lymphoma.
Toxoplasmosis CT • Plain CT –iso to hypodense with edema. • CECT – no enhancement, minimal, ring or nodular enhancement. MRI • T1WI –Iso to Hypointense but occasionally hyperintense due to hemorrhage which differentiate it from lymphoma. • T2WI –Hypo- to isointense and are surrounded by high-signal-intensity vasogenic edema. • T1W+C—Ring or nodular enhancement with sometimes an eccentric mural nodule (eccentric target sign).
Cryptococcosis • Most common fungus to involve brain. • Common symptoms-Headache, blurring of vision and seizure. • Cryptococcal meningitis: • Widened subarachnoid space by mucoid material & thickened leptomeninges. • Perivascular space involvement :M/c in HIV. • Expanded perivascular spaces by gelatinous material in BG, midbrain, dentate nucleus and subcortical WM. • Cryptococcomas: • Conglomeration of cryptococci & mucoid material.
Cryptococcosis Imaging features: • NECT-Sometimes hypodensity in BG. • CECT-No enhancement. • MR-Pseudocysts are hypointense on T1W images and hyperintense on T2W images suppress on FLAIR. • No enhancement on T1W+C is typical although mild pial enhancement is sometimes present. • D/D-Enlarge PVS, toxoplasmosis and TB.
Cryptococcosis • It may involve the meninges or present as cryptococcal masses • Meningeal involvement results in a basilar meningitis. • Diagnosis is made by detection of the cryptoccal antigen in the CSF via India ink preparation or fungal culture of the CSF • Neuroimaging studies are usually negative in cryptoccal meningitis. • Large amounts of trehalose relative to other metabolites on MRS defines as one markerthat can distinguish cryptococcus from other fungi.
CMV Infection • Common herpes virus that does not produce clinical disease in most people with an intact immune system. • CNS involvement typically assumes the form of meningoencephalitis or ventriculitis, but it can also take the form of myelitis, polyradiculitis, and retinitis.
cmv infection: • Radiological findings of CMV infections are: • Diffuse white matter disease. • Necrotizing ependymitis /ventriculitis. • Focal ring enhancing lesion.
CMV INFECTION • Imaging findings are frequently nonspecific and normal in CT/MR in most of the cases. • Demyelination can result in diffuse white matter abnormalities that appear as areas of hyperintensity on T2-weighted MR images. • Ependymitis and ventriculitis may show post contrast enhancement. • In rare cases ring-enhancing or space-occupying lesion may be seen.
PRIMARY CNS LYMPHOMA • Usually Non-Hodgkin`s(B cell type) lymphoma • Location: • Basal ganglia. • Periventricular. • Corpus callosum. • Presentation: • Seizures, Headaches, Focal neurological deficit.
PRIMARY CNS LYMPHOMA • IMAGING: • CT-Typically a solitary hyperdense mass on NECT however multifocal in 50% cases. • MR-Iso to hypointense on T1W and T2W image with diffusion restriction. • Enhancement pattern are variable homogenous/heterogenous/ring like. • Edema and mass effect in half of the lesion. • Increase choline peak on MRS and increase Thallium uptake on SPECT.
Primary CNS lymphoma High choline peak. Lactate peak in necrotic component.
Herpes viral encephalitis • Herpes simplex virus produces necrotizing encephalitis in the immunocompromised host that is more diffuse than the classic type. • Medial temporal , inferior frontal lobes and cingulategyrus m/c site. • Poorly defined areas of oedema with scattered foci of haemorrhagic signal are seen on imaging. • Diffusion restriction and post contrast enhancement are present.