Download
1 / 50
510 likes | 1.08k Vues
Immunodeficiency diseases. Zhang,Yunfeng. Immunologic disorders. Pathogens. Infectious Immunity. Immunity. Human. PID. Autoimmune Disease. Allergy. Tumor Immunity. Environment Material. Immunocompromised Host.

E N D
Immunodeficiency diseases Zhang,Yunfeng
Immunologic disorders Pathogens Infectious Immunity Immunity Human PID Autoimmune Disease Allergy Tumor Immunity Environment Material
Immunocompromised Host • Individual who has one or more defects in the body’s natural defense mechanisms which are sufficiently severe to predispose the host to life- threatening infection and high risk of autoimmune diseases, allergy and malignancy • Primary - PID, damage to anatomical barriers • Secondary - infection, tumor, drug, others • Physiology- Infants, aged
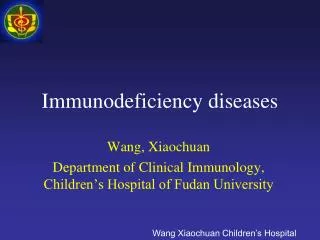
IgG from mother IgG of infant Development of Immunoglobulin IgG level of Infant 100% birth 6M
Schematic diagram of the exposure of microorganism during early life pathogens probiotics Full tern 6M Day care fetus
Period of susceptible children premature 6M Day care Full term
Management • Exclusion of PID • Clinical features • Frequency of infection • Severity • Complications • Follow up
Management • General medical care (prevention、nutrition、exercise) • Complication Treatment • Medication • Antibiotics • Immune regulator • Immunizations
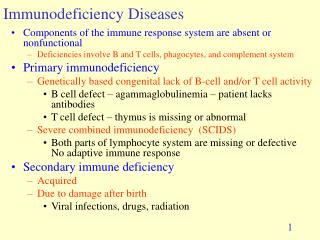
Primary Immunodeficiency Disease • A group of disorders characterized by an impaired ability to produce normal immune response. Most of these disorders are cased by mutations in genes involved in the development and function of immune organs, cells, and molecules. • Clinical features:Recurrent infection, high risk of autoimmune diseases, allergy and malignancy
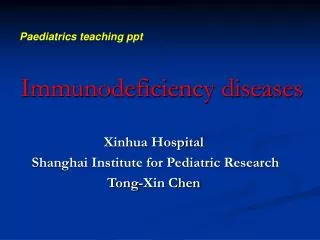
Complement Phagocyte 2% 18% 10% Cell mediated Antibody 50% 20% Combined
X-Linked Agammaglobulinemia (XLA) 1/ 100,000 Selective IgA Deficiency 1/10000 Severe Combined Immunodeficiency (SCID) 1/1,000,000 Chronic Granulomatous Disease (CGD) 1/1,000,000 100 500 10 10 Predictive patients number of PID in Shanghai
Classification (old) • Antibody(B cell) deficiency • T cell deficiency • Combined immunodeficiency • Phagocyte deficiency • Complement deficiency
Classification(new) • Combined Immunodeficiency • Predominantly antibody deficiency • Predominantly T-cell deficiency • Immunodeficiency syndromes • Phagocyte deficiency • Complement deficiency • Others
(4)第3、4咽囊综合征(DiGeorge anomaly) • (5)伴有白化病的免疫缺陷 • (a)Chediak Higashi 综合征 • (b)Griscelli综合征 • (6)x-连锁淋巴增殖综合征 • (7)家族嗜血细胞性淋巴组织病 • (8)X-连锁免疫调节异常、多种内分泌病、肠病综合征 • (9)自身免疫性多种内分泌病和外胚层发育不良 • (10) X-连锁免疫缺陷和外胚层发育不良 • 4.补体缺陷 • C1q,C1r,C4,C2,C3,C5,C6,C7,C8α,C8β,C9,C1抑制物,I因子,H因子,D因子,备解素等16种成分各自的缺陷 • 5.吞噬细胞数量和/或功能缺陷 • (1)严重先天性嗜中性粒细胞减少症 • (2)循环嗜中性粒细胞减少症 • (3)X-连锁嗜中性粒细胞减少症 • (4)白细胞粘附缺损1 • (5)白细胞粘附缺损2 • (6)Rac-2GTP酶缺陷 • (7)幼年型局限性牙周炎 • (8)特异性颗粒缺陷 • (9)Schwachman-Diamond综合征 • (10)慢性肉芽肿病(CGD) • (a)X-连锁CGD(细胞色素b的91kD链缺陷) • (b)常染色体隐性遗传(细胞色素b的22kD链缺陷或胞液因子的p47或p67缺陷) • (11) 嗜中性粒细胞葡萄糖-6-磷酸脱氢酶(G6PD)缺陷 • (12) 髓过氧化酶缺陷 • (13)白细胞分枝杆菌缺陷 • (a)IFN-γ受体缺陷 • (b)STAT-1缺陷 • (c)IL-12受体缺陷 • (d)IL-12缺陷 6.其它原发性免疫缺陷病 (1)原发性CD4T细胞缺陷 (2)IL-2缺陷 (3)多种细胞因子缺陷 (4)伴有或不伴有肌病的信号转导(transduction)缺陷 (5)伴肌病的钙流通缺陷 Up to 2007 more then 200 kinds of PID reported 1. 联合免疫缺陷 (1) 无T有B (a)X-连锁(γc缺陷) (b)常染色体隐性(Jak3缺陷) (c)IL7R缺陷 (d)CD45缺陷 (2)无T无B (a)RAG1/2缺陷 (b)Artemis缺陷 (c)腺苷脱氨酶(ADA)缺陷 (d)网状组织发育不良 (3)Omenn综合征 (4)X-连锁高IgM综合征 (5)CD40缺陷 (6)嘌呤核苷磷酸化酶(PNP)缺陷 (7)MHC Ⅱ类缺陷 (8)CD3γ或CD3ε缺陷 (9)CD8缺陷 (10)ZAP-70缺陷 (11)TAP-1缺陷 (12)TAP-2缺陷 (13)WHN缺陷 2.抗体缺损为主的免疫缺陷 (1)X-连锁无丙种球蛋白血症 (2)常染色体隐性无丙种球蛋白血症 (3)Ig重链基因缺失 (4)κ链缺陷 (5)选择性Ig缺陷 (a)IgG亚类缺陷 (b)IgA缺陷 (6)Ig水平正常的抗体缺陷 (7)常见变异型免疫缺陷 (8)婴儿暂时性低丙种球蛋白血症 (9)AID缺陷 3.其它确认的免疫缺陷综合征 (1)Wiskott-Aldrich综合征 (2)共济失调毛细血管扩张 (3)Nijmegen breakage
Case • 7-year-old Male,with 6 years history of recurrent coughing, fever, joints swollen and painful for 5 years. • The first onset of fever and coughing was at 10 months of age. Fever, coughing and left knee painful with move obstruction at 1 years and half age. After then on, the recurrent high fever, coughing and processing left knee functional obstruction exhibited every 2-3 months. Sometimes the symptoms were released by penicillin. The JRA, ankylosing spondylitis, rheumatic pneumonia were diagnosed successively and treatment with a series medicines. • A mother’s brother died as reccurent pnumonia and septicemia in infancy.
Case (continue) • Physical examination:T 39-40°C,malnutrition, small lymph nodes, absent tonsil • He had pneumonia and hepatosplenomegaly. Bilateral elbows, wrists, knees and ankle were swelling with tender, muscular atrophy.
Case (continue)–Lab investigation • RF negative , ESR:19mm/h, CRP:positive ANA negative,ENA negative, blood culture:negative • CD3: 83.77%, CD4: 31.89%, CD8: 46.98%, CD19: 0%. • IgG: 0.1g/L; IgA: 0.02g/L; IgM: 0.03g/L; IgE: 32IU/ml。CH50:90U/ml; C3: 189mg/dl • X-ray:periarticular soft-tissue swelling, periarticular osteopenia, and erosions with subluxation of the joint. Knees were deformation.
Characteristics • Male, onset at 10 months • Recurrent infection • Recurrent arthritis • Deceased serum Igs • Absence of circulating B cell
Case continue (Diagnosis) • Primary Immunodeficiency disease(X-linked agammaglobulinemia) • Juvenal Idiopathic Arthritis • Pneumonia • Diarrhea • Malnutrition
Antibody (B cell) Immunodeficiency • Hypogammaglobulinemia • X-linked agammaglobulinemia (XLA) • Transient Hypogammaglobulinemia • Common variable immunodeficiency disease (CVID) • Selective Ig deficiency • selective Ig A deficiency • selective Ig M deficiency • selective Ig G subclass deficiency
Clinical features of antibody immunodeficiency • Onset during 6-12 months of age • Recurrent Pyogenic bacterial infection (encapsulated invasive bacteria) • Pneumonia, media otitis, sinusitis, skin infection, meningitis, sepsis • Rare fungal, viral infection (but entericvirus) • High risk of allergy and autoimmune diseases
X-linked agammaglobulinemia (XLA; Bruton syndrom) • Gene defect: • Xq22 coded B cell tyrosin kinase ( Btk ) defect, XL • Mechanism: • B cell signal pass way disorder, development of B cell impaired
Clinical manifestations of XLA(1) • Onset at 6-12 month of age, male • Recurrent bacterial infection • Pyogenic encapsulated bacteria: • Streptococcus, Pneumoniae, Haemophilus influenzae, Staphylococcus aureus • Recurrent upper and lower respiratory infections, Pneumonia, media otitis, sinusitis, skin infection, meningitis, sepsis • 1/3 untreated patients with arthritis
Clinical features of XLA(2) • Physical examination: • Failure to thrive, small or absent tonsil, peripheral lymph nodes • Lab investigation: • IgG<2g/L, IgM、IgA、IgE reduced • Peripheral B cells absence, presence of pre or pro B cells in bone marrow • Normal T cell counts and function • Reduced monocyte BTK expression
Common variable immunodeficiency disease(CVID) • Pathogenesis: unclear
Clinical manifestations • Onset at any age, male and female • Recurrent Pyogenic bacterial infection • Higher risk for autoimmune diseases • Physical examination: • Part of patients tonsil and lymph node enlarge • Lab investigation: • IgG<3 g/L, most deficient in IgM、IgA、IgD、IgE • Most have near normal peripheral B cell • T cell numbers and function may be abnormal • Normal monocyte BTK expression
Clinical features of combined immunodeficiency • Onset age at early infants(4-5 months) • Recurrent infection with fungi, virus, bacteria, mycobacterium, protozoa • Opportunistic infections • Poor prognosis, early infant deaths • Severe infection after live virus vaccine and BCG • GVHD after blood transfusion • High risk of malignancy
X-linked Hyper IgM syndrome (HIGM) • Gene defect: T cell CD40 ligand defect, Chromosomal location Xq24-27, XL • Pathogenesis: Failure of B cell isotype switch
Clinical manifestations • Age of onset: first or second year of life • Male • Recurrent bacterial infections, other opportunistic infections include cytomegalovirus, mycobacteria, pneumocystis carinii • Lab investigation: Normal or elevated IgM level, decreased other Igs.
HIGM Isotype switch Pre B cell Immature B cellIgM (IgD) Mature B cell Igs HIGM patientT、Bcell cytokinesfailure ofIgisotype switch( IL-2 , 4, 10) normal T cells+patient B cells+cytokines Ig isotype seitch
Wiskott-Aldrich Syndrome • Gene defect: Xp11.22, Wiskott-Aldrich syndrome protein(WASp), XL • Clinical manifestations: X-linked, maleonset at early infant, eczema, thrombocytopenia, recurrent infectionlymphomas, autoimmune disease • Lab investigation: decreased IgM; often increased IgA and IgE
Ataxia-telangiectasia • Gene defect:mutation in A-T gene (ATM), AR • Clinical manifestations • Ataxia • Telangiectasia • Recurrent infections • Malignancies • X-ray sensitivity
DiGeorge anomaly • Genetic defect: located at 22q11, AR • Contiguous gene syndrome that affect multiple organs during early embryogenesis • Thymic hypoplasia • Hypocalcaemia • Cardiac abnormalities • Cleft palate • Abnormal facies
Chronic granulomatous disease(CGD) • Genetic defect: • gp 91 phox, XL • p22 phox; p47 phox; p67 phox, AR • 2/3 onset before 1 year, most under 6 months of age • Skin infection and abscess
IL-12RB1 deficiency • Case: • 1 years old girl with BCG infection from first month after got BCG vaccine. • With very limited effects with the anti-tuberculosis therapy • Immunology evaluation is normal
IL-12RB1 gene mutation Intron 15 (+2) T>G mutation Intron 15 (+2) T/G carrier Intron 15 (+2) T/G carrier
IFNg/IL-12 pathway IL-12 p40 p35 b1 b2 IL-12 R STAT4 Macrophage T/NK cell STAT1 IFN-g R IFN-g R IFN-g Other factors, e.g., TNF-a
It is now clear that most, if not all individuals, suffer from at least one PID, the clinical expression of which depends on exposure to ad hoc environmental factors, infectious or otherwise. Casanova JL, Abel L. SCIENCE 2007(317): 617-619
Treatment • General management • Immunoglobulin • Replacement therapy • Transplantation, others
General management • Diet • Avoidance of pathogens (“germ-free” care) • Antibiotics • Use in acute illness • Prophylactic • Avoid whole blood transfusion in combined immunodeficiency disorder • Avoid live virus vaccines and BCG
Immunoglobulin replacement • Treatment of severe antibody disorders • Intramuscular • 0.1g/kg/m • Intravenous • 0.4-0.6g/kg/m
Immunoglobulin replacement adverse effects • Local reactions: intramuscular gammaglobulin, tenderness, abscesses, fibrosis • Systemic reaction: Fever, chills, nausea, vomiting; anaphylactic reaction are unusual
Specific treatment for cellular deficiency • Bone marrow transplantation • Replacement therapy • Enzyme replacement • Gene therapy • Thymic hormones • Cytokines • Fetal thymus transplantation
Specific treatment of phagocytic disorders • Interferon gamma for CGD • Granulocyte transfusion