An Innovative Strategy for Lean Scheduling and Same Day Access
770 likes | 1.12k Vues
An Innovative Strategy for Lean Scheduling and Same Day Access. Carrie Nelson, MD, MS, FAAFP Medical Director, Your Healthcare Plus Brenda K. Fann, MD, FAAFP Program Director Rush-Copley Family Medicine Residency Program. Learning Objectives.

An Innovative Strategy for Lean Scheduling and Same Day Access
E N D
Presentation Transcript
An Innovative Strategy for Lean Scheduling and Same Day Access Carrie Nelson, MD, MS, FAAFP Medical Director, Your Healthcare Plus Brenda K. Fann, MD, FAAFP Program Director Rush-Copley Family Medicine Residency Program
Learning Objectives Describe and contrast three models of appointment scheduling Understand the effects of these models on office efficiency, satisfaction, and continuity Use the Lean Model to find and eliminate office inefficiencies related to same-day access Learn how to implement a new same day access system in your office
Outline • Explain the various models of scheduling • Introduce our novel, never-described-before strategy for same day access • Present our data after one year of implementation • Discuss the “ups” and “downs” of our strategy
Access Options The Ups And Downs
Various Scheduling Options • Traditional Scheduling • Advanced (Open) Access • The Toyota Way—WIA
Traditional Scheduling“Carve-Out Model” • Appointments made in advance for predictable needs • Multiple “rules” about how to schedule i.e. # of paps in a day, several appointment types/lengths • Some appointments “frozen” for same-day needs • When frozen appointments run out…
Traditional Scheduling Patients call to schedule anticipated needs in advance Schedulers work some into slots that are available—same day, next week, next month When appts run out schedulers pass acute/urgent needs on to the triage nurse Patients call with unpredictable needs The Cycle of Despair
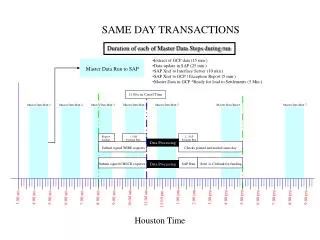
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE Front desk transfers to Triage Sun night person calls as told on Monday AM Triage Nurse on another call, talking to doctor, etc WASTE WASTE Triage Nurse has some same-day appts available on Monday Patient leaves message WASTE WASTE Not all appts needed so some days they go unused Triage Nurse calls back WASTE All acute appts gone by 10:30 am WASTE Pt not available; already in ED Talk to doctor—figure out how to see them, send to ED, defer to Tues WASTE
Illusion of Control Predictability? Daily fretting about appt availability by schedulers and triage Patient dissatisfaction with access Waste in the Traditional Scheduling Model:The Ups and Downs The Cycle of Despair
Data on Triage Nurse Activities • Calls received • Appointments made Net result
Net Result of Triage Nurse Activities: One Week in October 78% of the time an appointment was made 11% of the time phone advice was given 2% of the time a prescription was initiated 9% of the time the patient had a question for the doctor
Advanced Access P r o g r e s s
Advanced Access Model • Patients are seen on the day they call regardless of the reason for the visit • Start the day with up to 100% of schedule unfilled • Some practices allow for “good” backlog so that patients can schedule predictable needs in advance • A commitment to… “Doing today’s work today”
Key Elements of Advanced Access • Understand your demand • Match your supply with demand • Establish generic appointment types • “Max-pack” visits • Strive for continuity
Advanced (Open) Access Scheduling Patients Call for anticipated/routine needs or unpredictable/acute needs Scheduler has a schedule that is X % open at the start of the day Appts are made regardless of reason for the visit Contingency plans for vacations, days off, etc.
Better patient satisfaction with access Enhanced continuity Fewer no-shows Decreased waste Overall enhanced revenue The painful backlog reduction phase Can be hard to maintain Daily unpredictability collides with the realities of provider and staff lives At it’s extreme, it interferes with the Planned Care Model “Max-packing” can decrease revenue opportunities Potential for non-sensical work-arounds Advanced Access: The Ups and Downs
Recommended Features of Any Appointment System • Limit appointment types • Understand the demand for appointments • Make sure each physician has a manageable panel size (~2000 patients) • Maximize today’s visit? • Decide (preferably with patient input) how you define and measure continuity
New & Improved Access P r o g r e s s
What were our goals? Provide enhanced access as per PCMH principle Eliminate the patients’ barriers for acute access Use the Lean model to avoid multiple areas of waste & eliminate inefficencies Improve patient, staff and physician satisfaction Maintain continuity Decrease phone calls and downstream demand (i.e., ER visits)
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE Front desk transfers to Triage Sun night person calls as told on Monday AM Triage Nurse on another call, talking to doctor, etc WASTE WASTE Triage Nurse has some same-day appts available on Monday Patient leaves message WASTE WASTE Not all appts needed so some days they go unused Triage Nurse calls back WASTE All acute appts gone by 10:30 am WASTE Pt not available; already in ED Talk to doctor—figure out how to see them, send to ED, defer to Tues WASTE
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE Front desk transfers to Triage Triage Nurse on another call, talking to doctor, etc WASTE WASTE Triage Nurse has some same-day appts available on Monday Patient leaves message WASTE WASTE Not all appts needed so some days they go unused Triage Nurse calls back WASTE All acute appts gone by 10:30 am WASTE Pt not available; already in ED Talk to doctor—figure out how to see them, send to ED, defer to Tues WASTE
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE Triage Nurse on another call, talking to doctor, etc WASTE WASTE Triage Nurse has some same-day appts available on Monday Patient leaves message WASTE WASTE Not all appts needed so some days they go unused Triage Nurse calls back WASTE All acute appts gone by 10:30 am WASTE Pt not available; already in ED Talk to doctor—figure out how to see them, send to ED, defer to Tues WASTE
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE Triage Nurse on another call, talking to doctor, etc WASTE WASTE Patient leaves message WASTE WASTE Not all appts needed so some days they go unused Triage Nurse calls back WASTE All acute appts gone by 10:30 am WASTE Pt not available; already in ED Talk to doctor—figure out how to see them, send to ED, defer to Tues WASTE
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE Triage Nurse on another call, talking to doctor, etc WASTE WASTE Patient leaves message WASTE WASTE Triage Nurse calls back WASTE All acute appts gone by 10:30 am WASTE Pt not available; already in ED Talk to doctor—figure out how to see them, send to ED, defer to Tues WASTE
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE Triage Nurse on another call, talking to doctor, etc WASTE WASTE Patient leaves message WASTE WASTE Triage Nurse calls back WASTE WASTE Pt not available; already in ED Talk to doctor—figure out how to see them, send to ED, defer to Tues WASTE
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE Triage Nurse on another call, talking to doctor, etc WASTE WASTE Patient leaves message WASTE WASTE Triage Nurse calls back WASTE WASTE Pt not available; already in ED WASTE
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE WASTE WASTE Patient leaves message WASTE WASTE Triage Nurse calls back WASTE WASTE Pt not available; already in ED WASTE
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE WASTE WASTE WASTE WASTE Triage Nurse calls back WASTE WASTE Pt not available; already in ED WASTE
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE WASTE WASTE WASTE WASTE WASTE WASTE Pt not available; already in ED WASTE
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WASTE WASTE WASTE WASTE WASTE WASTE WASTE WASTE
Old System—Acute Appointment People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM
System—Acute Appointment New Old People call on Sunday Night with acute symptoms New pts with acute symptoms call Mon AM WIA-aware patients walk-in Monday AM WIA
WIA System Dr. Fann’s Schedule 8:30 AM 9:00 AM 9:30 AM 10:00 AM A. Smith Well Woman Exam 10:30 AM B. Smith Diabetic & HTN F/U 11:00 AM C. Smith Headaches 11:30 AM D. Smith Wrist Pain 12:00 PM Lunch Break M. Smith Cough Patients walk-in between 8:30 – 9:30 AM N. Smith Wheezing O. Smith Rash P. Smith Ear Ache Q. Smith ? UTI
X The Cycle of Despair
Our WIA Policy…at First Established patients only Minor, urgent, acute problems Quick appointments – 10 minutes or so Not for chronic disease follow-up, gynecological issues, well child exams, general exams, pap smears, long-term unresolved issues Patients may have to wait, but will be seen that clinic session Follow-up with regular doctor for other issues
How did we start it? Consulted our Marketing and Advertising Department Informed patients Posted flyers in the FMC Described in the patient newsletter Educated Staff and Physicians Clear and written policy Discussed at our All Center Meeting Templated the schedule accordingly
Our FMC 12 residents 2-4 doctors in clinic at a time Per MGMA benchmarking standards Approximately 2.73 FP FTE’s (with OB) based on our volume Approximately 3.8 FP FTE’s based on hours of clinic operations Panel size of 7,054 patients 12,131 total patient visits (FY08) 13,482 total patient visits (FY09)
How many patients will show up? Which days will be busier? Will mornings or afternoons be busier? How much time should be allowed for WIA? Will patients be lining up hours before opening? How do we anticipate and plan??? Should we do this??? ? ? ? ? ? ? ? ? ? ? ?
Patient Volume by Month Do I have H1N1?? Average of 178 patients per month for FY09 Average of 235 patients per month thus far FY10