Tract GAstrointestinal
710 likes | 916 Vues
Aging and. Tract GAstrointestinal. What IS Aging?. Practically …. Aging = reduced tissue/physiological function. Aging = increased susceptibility to disease (age-related diseases). Aging = decreased resistance to stress (physical and psychological). Why do we age --- GENES.

Tract GAstrointestinal
E N D
Presentation Transcript
Aging and TractGAstrointestinal
Practically …. Aging = reduced tissue/physiological function Aging = increased susceptibility to disease (age-related diseases) Aging = decreased resistance to stress (physical and psychological)
Why do we age --- GENES Genes determine species-specific life span (LAGs) (e.g., mice, monkeys, humans, tortoises) Genes determine differences among individuals within a species (e.g., big/small noses) (genetic polymorphisms)
Species-specific longevity genes Flies (Drosophila melanogaster) Nematodes (Caenorhabditis elegans) Mice (Mus musculus) Humans (Homo sapiens) Galapagos turtles (Geochelone elephantopus) Life spans ranging from 2-3 weeks to 100-200 years!
50 Years 18 Months AGING in MICE AND MEN MICE HUMANS Fitness Disease (Cancer, osteoporosis, diabetes, etc.) AGE (log) Mice and Humans are 97% genetically similar!
Species-specific longevity genes What are the genes that determine why mice live <4 years, whereas humans live >100 years? Potentially big pay-off, but complicated by development/evolution
Individual longevity genes (polymorphisms) Smaller pay-off, but possibly amenable to intervention (environment, life style, drugs??)
Aging Can we do Intervention.?
DIET Eat well, but not too much! Food ----> simple molecules + oxygen (mitochondria) ----> energy FOOD ---> ENERGY Oxygen metabolism ----> damaging byproducts (ROS, oxidative stress) Anti-oxidant defenses good, but not perfect (different among species) OPTIMAL food = less ROS, less damage, more defenses longer lifespans!
DIET DIET CALORIC RESTRICTION GOOD NEWS! 30-40% calorie restriction without malnutrition extends HEALTHY lifespan 40-50% (worms, flies, mice, rats -- maybe monkeys) BAD NEWS! Life SEEMS longer!! (let's develop that CR pill)
EXERCISE Yes, yes, yes ….. (but not too much) Exercise ---> healthier muscles, May be prevent telomere shortening .greater fitness Greater protection from oxidative stress! (not such a paradox, anti-oxidant defenses)
Think good thoughts! Avoid undue stress Physiological stress: Stress hormones, a double edged sword Physical stress: Overwhelm cellular defense mechanisms
Why do we age --- PAST ENVIRONMENT Genes evolve in response to environment This is REALLY why we age!
Aging before cell phones …….. "Protected" Environment (climate control, biomedical intervention etc.) 100% SURVIVORS "Natural" Environment (hazards, predators, infection, etc.) HUMANS: MICE: 4 mos 40 yrs 80 yrs 3-4 yrs AGE
GOOD NEWS! If we keep our "protected" environment, we WILL evolve longer life spans! BAD NEWS! It's going to take a LONG time!
Sooo…. What's to be done about aging now? Optimize present environment New therapies on the horizon! •Cell based therapies •Drug based therapies Support basic research in aging!
Individual longevity genes Most identified so far are disease-susceptibility genes its role in several biological processes not directly related to lipoprotein transport, including Alzheimer's disease (AD), immunoregulation, and cognition.(e.g., ApoE4) Solution = preventive drugs Healthy centenarian studies are underway! Solution = ??????
Cell based therapies Stem cells! • embryonic • adult • nuclear transplant (cloning) Telomerase! • increase cell divisions • anti-cancer therapy
Drug-based therapies Anti-oxidants, mitochondrial protectors, etc. Hormones! • growth hormone • insulin/IGF (lessons from worms and flies) • estrogen CR mimetics!
AgingDefinition Aging is the progressive, universal decline first in functional reserve and then in function that occurs in organisms over Aging is heterogeneous. It varies widely in different individuals and in different organs within a particular individual. Aging is not a disease; however, the risk of developing disease is increased, often dramatically, as a function of age. The biochemical composition of tissues changes with age; physiologic capacity decreases, the ability to maintain homeostasis in adapting to stressors declines, and vulnerability to disease processes increases with age .
Biology of Aging As we age, we become increasingly unlike one another. For any variable one can measure, the variation in the distribution of values in a population increases with age. While the mean value may trend up or down, the age-related increase in the range of values is striking testimony to the diverse manifestations of the aging process. In addition, homeostatic mechanisms are slower to respond to stressors and take longer to restore normal function as we age. The ability to maintain stable function in the face of a change in the environment is called allostasisand it declines with age.
Demography of Aging Improvements in environmental (e.g., clean water and improved sanitation) and behavioral (nutrition, reduced risk exposures) factors and the treatment and prevention of infectious diseases are largely responsible for the 30-year increase in life expectancy since 1900. In the United States, by 2030, 1 person in 5 will be >65 years.
Global Aging At present 59% of older adults live in the developing countries of Africa, Asia, Latin America, the Caribbean, and Oceania. The developed world has the largest absolute number of older adults and is experiencing the largest percentage increase.
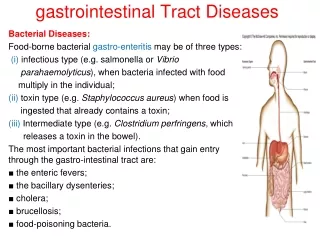
Gastrointestinal Disorders Gastrointestinal (GI) disorders represent the third cause of consultations by general practitioners among subjects older than 65 years in Western countries.
Gastrointestinal Disorders Age-related anatomical and physiologic changes occur in the major organ systems, affecting functions as diverse as swallowing and hepatic and renal clearance of therapeutic drugs. Because of these factors, and because older patients are more likely to be receiving multiple drugs for concomitant illness, they are more prone to drug-drug interactions and to medication-induced injury of the esophagus and stomach. In addition, several gastrointestinal disorders, notably gastroesophageal reflux and peptic ulcer disease, are commonly seen in the elderly. J Clin Gastroenterol. 1991;13 Suppl 2:S65-75Bozymski EM, Isaacs KL Department of Medicine, University of North Carolina, Chapel Hill 27599-7080
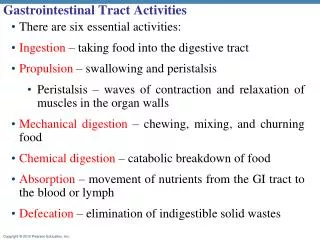
Objectives • Define age-related changes in the gastrointestinal tract • Discuss common G.I. problems associated with aging • Describe the risk factors for gastro-esophageal reflux disease • Describe the risk factors for peptic ulcer development • List the causes of diarrhea and fecal incontinence in the elderly
Epidemiology • Over 35 million people aged > 65 years in the United States • 12% of the 2003 US population were older than 65 • 18.3 million aged 65-74 • 12.9 million aged 75-84 • 4.7 million aged ≥ 85 • 35% to 40% of geriatric patients will have at least 1 GI symptom in any year • Common problems in this age group include constipation, fecal incontinence, diarrhea, irritable bowel syndrome (IBS), reflux disease, and swallowing disorders Hall KE, et al. Gastroenterology. 2005;129:1305-1338. He W, et al. 65+ in the US: 2005. US Census Bureau Web site. Available at: http://www.census.gov/prod/2006pubs/p23-209.pdf. Accessed 11/30/06.
Increase in the Number of Persons Aged 65+ Years in the United States 72 (20%) Number (millions) Percent of population 55 (16%) 40 (13%) Population 35 (12%) 31 (13%) 26 (11%) 20 (10%) 17 (9%) 12 (8%) 9 (7%) 7 (5%) 5 (5%) 4 (4%) 3 (4%) Year The “Age Wave” He W, et al. 65+ in the US: 2005. US Census Bureau Web site. Available at: http://www.census.gov/prod/2006pubs/p23-209.pdf. Accessed 11/30/06.
Motility an GI tract Normal aging is associated with significant changes in the function of most organs and tissues. In this regard, the gastrointestinal More important is the impact of various age-related diseases on gastrointestinal motility in the elderly: for example, long-standing diabetes mellitus may reduce gastric emptying in up to 50% of patients; depression significantly prolongs whole-gut transit time; hypothyroidism may prolong oro-caecal transit time; and chronic renal failure is associated with impaired gastric emptying. In addition, various, frequently used drugs in the elderly cause disordered gastrointestinal motility. These drugs include anticholinergics, especially antidepressants with an anticholinergic effect, opioid analgesics and calcium antagoniststract is no exception.
Gastrointestinal Disorders Available data allow the conclusion to be drawn that impaired intestinal motility, as evidenced by attenuated migrating motor complex activity, results in bacterial overgrowth.
GI Motility pristalsism and Migratory Myo electric complex
Gastrointestinal Disorders • Heart disease, cancer, and stroke have become the leading "killers" among older adults, while deaths due to infection have decreased. Adults surviving into late life suffer from high rates of chronic illness; 80 percent have at least one and 50 percent have at least two chronic condition. There is a strong association between the presence of geriatric syndromes (cognitive impairment, falls, incontinence, vision or hearing impairment, low body mass index, dizziness) and dependency in activities of daily living
Geriatric diseases of the upper digestive tract During aging, secretion and motility of the upper GI tract slow down. The reduction of these functions, however, does not create complaints. In the higher age groups, a number of symptoms from age-dependent diseases occur more frequently, e.g., dysphagia in response to cerebral ischemia, or disturbed gastric emptying caused by diabetic visceral neuropathy. Moreover, certain GI diseases occur more often in the elderly, e.g., chronic atrophic gastritis, NSAR-induced gastric ulcers, malignancies, and others. In contrast, almost nothing is known about diseases or symptoms of the GI tract that might be specific for the elderly. With only a few exceptions, there are no age-dependent clinical differences. Nevertheless, intestinal diseases often develop more rapidly and the mortality is higher in the elderly than in younger people. Z Gerontol. 1992 Sep-Oct;25(5):286-8.
Age-Related Changes in the Gastrointestinal Tract • Areas identified as important to aging are: • Pathophysiology of swallowing disorders • Esophageal reflux • Dysmotility symptoms • GI immunobiology • Cellular mechanisms of neoplasia in the GI tract • Decreased visceral sensitivity Motility Hormone responsiveness Visceral sensitivity Drug metabolism Liver sensitivity to stress Pancreas: Structure and function Immunity Lithogenic bile Colonic function Hall KE, et al. Gastroenterology. 2005;129:1305-1338.