Download
1 / 80
800 likes | 855 Vues
Learn about hormones, chemical messengers that regulate cell functions. Explore hormone release control, classes, actions, and receptor specificity.

E N D
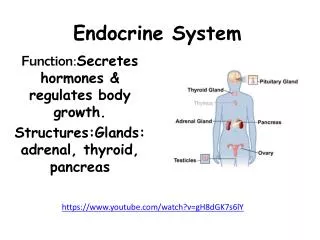
Let’s define some more - Define Hormone • The term hormone is derived from a Greek verb meaning – to excite or arouse • Hormone is a chemical messenger that is released in one tissue (endocrine tissue/gland) and transported in the bloodstream to reach specific cells in other tissues • Regulate the metabolic function of other cells • Have lag times ranging from seconds to hours • Tend to have prolonged effects • Hormone actions must be terminated – how?
Endocrine versus Nervous system • Both use chemical communication • Both are being regulated primarily by negative feedback • Released in synapse • Close to target cells • Signal to release by action potential • Short live effect • Crisis management Neurotransmitters Hormones • Released to bloodstream • Can be distant from target cells • Different types of signal • Long term effect • Ongoing processes
Control of Hormone Release • Blood levels of hormones: • Are controlled by negative feedback systems • Vary only within a narrow desirable range • Hormones are synthesized and released in response to: • Humoral stimuli • Neural stimuli • Hormonal stimuli
Humoral Stimuli • Secretion of hormones in direct response to changing blood levels of ions and nutrients • Example: concentration of calcium ions in the blood • Declining blood Ca2+ concentration stimulates the parathyroid glands to secrete PTH (parathyroid hormone) • PTH causes Ca2+ concentrations to rise and the stimulus is removed
Neural Stimuli • Neural stimuli – nerve fibers stimulate hormone release • Preganglionic sympathetic nervous system (SNS) fibers stimulate the adrenal medulla to secrete catecholamines Figure 16.5b
Hormonal Stimuli • Hormonal stimuli – release of hormones in response to hormones produced by other endocrine organs • The hypothalamic hormones stimulate the anterior pituitary • In turn, pituitary hormones stimulate targets to secrete still more hormones
Classes of Hormones – by chemical structure • Hormones can be divided into three groups • Amino acid derivatives • Peptide hormones • Lipid derivatives
Chemical structure AA derivatives Peptides lipids small proteins: GH,PRL • Tyrosine: • Thyroid hormones • Catecholamines (Epinephrine, norepinephrine • Tryptophan: • Dopamine, serotonin, melatonin Eicosanoid: prostaglandins Glycoproteins: TSH, LH, FSH short peptides: ADH, OT steroids
Distribution of Hormones in bloodstream • Hormones that are released into the blood are being transported in one of 2 ways: • Freely circulating • Bound to transport protein
Distribution of Hormones in bloodstream • Freely circulating (most hormones) • Hormones that are freely circulating remain functional for less than one hour and some as little as 2 minutes • Freely circulating hormones are inactivated when: * bind to receptors on target cells * being broken down by cells of the liver or kidneys * being broken down by enzymes in the plasma or interstitial fluid • Bound to transport proteins – thyroid and steroid hormones (>1% circulate freely) • Remain in circulation longer
Hormones: Classification Table 7-1
Target Cell Specificity • Hormones circulate to all tissues but only activate cells referred to as target cells • Target cells must have specific receptorsto which the hormone binds • These receptors may be intracellular or located on the plasma membrane • Hormone exert their effects on target cells at very low bloodconcentrations (ng-10-9 gr; pg-10-12 gr) • In most systems the maximum biological response is achieved at concentrations of hormone lower than required to occupy all of the receptors on the cell (spare receptors). • Examples: • insulin stimulates maximum glucose oxidation in adipocytes with only 2-3% of receptors bound • LH stimulates maximum testosterone production in Leydig cells when only 1% of receptors are bound
Receptors for hormones are located: • on the cell membranes of target cells • In the cytoplasm or nucleus • Can you tell which hormone group/s will have their receptors on the cell membrane and which in the cytoplasm?
Mechanisms of Hormone Action • Two mechanisms, depending on their chemical nature • Water-soluble hormones (all amino acid–based hormones except thyroid hormone) • Cannot enter the target cells • Act on plasma membrane receptors • Coupled by G proteins to intracellular second messengers that mediate the target cell’s response • Lipid-soluble hormones (steroid and thyroid hormones) • Act on intracellular receptors that directly activate genes
Receptors on the cell membrane • Hormones do not induces changes in cell activity directly but via the induction of the appearance and action of other agents • Hormones are referred to as first messengers and the agents that are activated by the hormones are called second messengers. • All amino-acid hormones (with exception of the thyroid hormone) exert their signals through a second messenger system: • cAMP • PIP
Amino Acid-Based Hormone Action: cAMP Second Messenger • Hormone (first messenger) binds to its receptor, which then binds to a G protein • The G protein is then activated • Activated G protein activates the effector enzyme adenylate cyclase • Adenylate cyclase generates cAMP (second messenger) from ATP • cAMP activates protein kinases, which then cause cellular effects
Extracellular fluid 1 Hormone (1st messenger)binds receptor. Adenylate cyclase G protein (GS) 5 cAMP acti-vates proteinkinases. Receptor Activeproteinkinase GDP Inactiveprotein kinase 2 3 4 Receptoractivates Gprotein (GS). G proteinactivatesadenylatecyclase. Adenylatecyclaseconverts ATPto cAMP (2ndmessenger). Hormones thatact via cAMPmechanisms: Triggers responses oftarget cell (activatesenzymes, stimulatescellular secretion,opens ion channel,etc.) GlucagonPTHTSHCalcitonin EpinephrineACTHFSHLH Cytoplasm Figure 16.2, step 5
Amino Acid-Based Hormone Action: PIP-Calcium • Hormone binds to the receptor and activates G protein • G protein binds and activates phospholipase • Phospholipase splits the phospholipid PIP2 into diacylglycerol (DAG) and IP3 (both act as second messengers) • DAG activates protein kinases; IP3 triggers release of Ca2+ stores • Ca2+ (third messenger) alters cellular responses
Amino Acid-Based Hormone Action: PIP Mechanism Extracellular fluid Hormone DAG 1 4 5 Active protein kinase C 2 3 PIP2 GTP GTP Receptor Gq Inactive protein kinase C GDP GTP IP3 Phospholipase C Catecholamines TRH ADH GnRH Oxytocin Triggers responses of target cell 5 Endoplasmic reticulum 6 Cytoplasm Ca2+ Ca2+- calmodulin Figure 16.3
Steroid Hormones: Action 1 Most hydrophobic steroids are bound to plasma protein carriers. Only unbound hormones can diffuse into the target cell. Blood vessel Steroid hormone Cell surface receptor 2a Rapid responses 1 2 Steroid hormone receptors are in the cytoplasm or nucleus. 2 Protein carrier Nucleus 2a Some steroid hormones also bind to membrane receptors that use second messenger systems to create rapid cellular responses. Cytoplasmic receptor Nuclear receptor DNA Interstitial fluid 3 The receptor-hormone complex binds to DNA and activates or represses one or more genes. 3 Endoplasmic reticulum Transcription produces mRNA Cell membrane 4 Activated genes create new mRNA that moves back to the cytoplasm. 5 4 New proteins Translation 5 Translation produces new proteins for cell processes. Figure 7-7, steps 1–5
http://arbl.cvmbs.colostate.edu/hbooks/pathphys/endocrine/moaction/change.htmlhttp://arbl.cvmbs.colostate.edu/hbooks/pathphys/endocrine/moaction/change.html
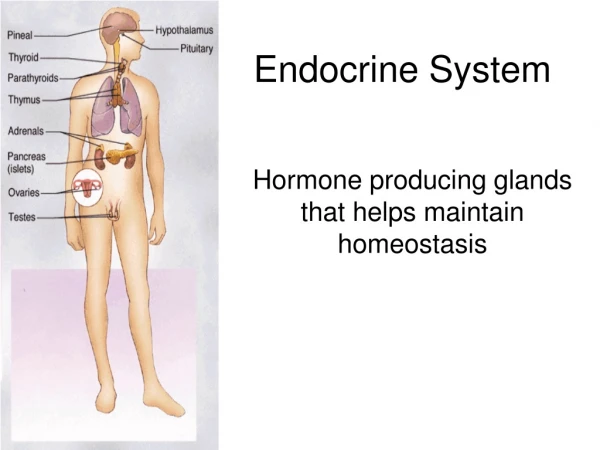
How will we approach the endocrine system? • We will group them according to their function in the body: • Hormones that control blood glucose levels • Hormones that control minerals and water balance • Hormones that are involved in growth and metabolism • Hormones and the reproductive system
Hormones that control blood glucose levels • The levels of blood glucose are closely monitored to maintain relative constant levels. • What hormones control the glucose levels? • Which organs are responsible to produce these hormones?
Pancreas structure Exocrine pancreas (99% of volume) Cells (pancreatic acini) forming glands and ducts that secrete pancreatic fluid and enzymes with digestive function Endocrine pancreas (1%) Small groups of cells scattered in clusters (pancreatic islets) that secrete hormones
Insulin • A 51-amino-acid protein consisting of two amino acid chains linked by disulfide bonds • Insulin is released when glucose levels exceed normal levels (70-110 mg/dl) http://www.chemistryexplained.com/images/chfa_02_img0437.jpg
Effects of Insulin Binding to its receptors • Insulin facilitates entry of glucose cells by binding to a membrane receptor • The complex insulin-receptor make a specific carrier protein (GLUT4) available • Once at the cell surface, GLUT4 facilitates the passive diffusion of circulating glucose down its concentration gradient into cells. • Receptors for insulin are present in most cell membranes (insulin-dependant cells) • Cells that lack insulin receptors are cells in the brain, kidneys, lining of the digestive tract and RBC (insulin-independent cells). • Those cells can absorb and utilize glucose without insulin stimulation.
Effects of Insulin • Acceleration of glucose uptake as a result from an increase of the number of glucose carrier proteins • Acceleration of glucose utilization and increased ATP production • Stimulation of glycogen formation in the liver and muscle cells • Inhibits glycogenolysis (break down of glycogen) and gluconeogenesis (glucose building) • Stimulation of amino acid absorption and protein synthesis • Stimulation of triglyceride formation in adipose tissue • As a result glucose concentration in the blood decreases
Glucagon • Released by alpha cells • A 29-amino-acid polypeptide hormone that is a potent hyperglycemic agent (what does it mean?) • it promotes: • Glycogenolysis – the breakdown of glycogen to glucose in the liver and skeletal muscle • Gluconeogenesis – synthesis of glucose from lactic acid and noncarbohydrates in the liver • Release of glucose to the blood from liver cells • breakdown of triglycerides in adipose tissue
Other hormones that control glucose levels • Glucocorticoids from the adrenal gland
Adrenal (Suprarenal) Glands • Structurally and functionally, they are two glands in one • Adrenal medulla – neural tissue; part of the sympathetic nervous system • Adrenal cortex - three layers of glandular tissue that synthesize and secrete corticosteroids
Adrenal Cortex • Synthesizes and releases steroid hormones called corticosteroids • Different corticosteroids are produced in each of the three layers • Zonaglomerulosa – glomerulus- little ball. Secretes mineralocorticoids – main one aldosterone • Zonafasciculata– glucocorticoids (chiefly cortisol) • Zonareticularis – gonadocorticoids (chiefly androgens)
Zonafasciculata - Glucocorticoids (Cortisol/hydrocortisone) • Main hormones secreted are the Cortisol/hydrocortisone and small amounts of corticosterone • Glucocorticoids often called the body’s stress hormones • While adrenaline is responsible for rapid metabolic responses the glucocorticoids are responsible for long-term stress: • Glucocorticoids accelerate the rates of glucose synthesis and glycogen formation – especially in the liver • Adipose tissue responds by releasing fatty acids into the blood and the tissues start to utilize fatty acids as source of energy - glucose-sparing effect (GH has similar effect and will be discussed later) • Clucocorticoids also have anti-inflammatory effect – inhibit the activities of WBC (use?)
Pathway For the Control of Cortisol Secretion Circadianrhythm Stress Hypothalamus CRH long-loop negative feedback Anteriorpituitary ACTH Adrenalcortex Cortisol Immunesystem Adiposetissue Muscle Liver Functionsuppressed Gluco-neogenesis Proteincatabolism Lipolysis Figure 23-3
Diabetes Mellitus (DM) • Two types: • Type I results from the destruction of beta cells and the complete loss of insulin (hypoinsulinemia) • Type II is the most common type (90%) and is a result of decrease sensitivity of cells to insulin (insulin resistance). Type II is accompanied by hyperinsulinemia (what is that? Why?). • Type II is associated with excess weight gain and obesity but the mechanisms are unclear. • Other reasons that were associated with type II diabetes: pregnancy, polycystic ovary disease, mutations in insulin receptors and others
Type 1 and Type 2 Diabetes Mellitus Table 24.1
Diabetes Mellitus (DM) effects • Increase in blood glucose due to diabetes causes • Increase in glucose loss in urine • Dehydration of cells – since glucose does not diffuse through cell membrane and there is an increase in osmotic pressure in the extracellualr fluid. • In addition, the loss of glucose in the urine causes osmotic diuresis - decrease in water reabsorption in the kidney. • The result is • Polyuria – huge urine output and dehydration. • Polydipsia – excessive thirst
Diabetes Mellitus (DM) effects • Polyphagia – excessive hunger and food consumption because cells are starving • Damage to blood vessels and poor blood supply to different tissues • Increase use of lipids as a source of energy by the cells and increase release of keto bodies – ketosis and changes of blood pH (acidosis). That leads to increased respiratory rate
Hormones that control minerals and water • We will see the different glands that control: • Sodium – Adrenal gland • Which layer and what hormone group? • Calcium – Thyroid and parathyroid • Water - hypothalamus
Zonaglomerulosa – Mineralocorticoids • Aldosterone secretion is stimulated by: • Rising blood levels of K+ • Low blood Na+ • Decreasing blood volume or pressure
Zonaglomerulosa- Mineralocorticoids • The mineralocorticoids are steroids that affect the electrolytes composition of the body extracellular fluids. • Aldosterone – most important mineralocorticoid • Maintains Na+ balance by reducing excretion of sodium from the body • Stimulates re-absorption of Na+ by the kidneys • Prevents the loss of Na+ by the kidneys, sweat glands, salivary glands and digestive system • As a result of Na+ reabsorption there is also water reabsorption • The retention of Na+ is accompanied by a loss of K+
Protein hormones that control calcium • Thyroid gland – calcitonin • Parathyroid gland – PTH • PTH—most important hormone in Ca2+ homeostasis
Effects of Parathyroid Hormone • PTH release increases Ca2+ in the blood: • Stimulates osteoclasts to digest bone matrix • Enhances the reabsorption of Ca2+ and the secretion of phosphate by the kidneys • Increases absorption of Ca2+ by intestinal mucosal • Rising Ca2+ in the blood inhibits PTH release (what type of control is it?) • The antagonist is the Calcitonin secreted by the thyroid gland
Hypocalcemia (low blood Ca2+) stimulates parathyroid glands to release PTH. Rising Ca2+ in blood inhibits PTH release. Bone 1 PTH activates osteoclasts: Ca2+ and PO43Sreleased into blood. Kidney 2 PTH increases Ca2+reabsorption in kidney tubules. 3 PTH promotes kidney’s activation of vitamin D, which increases Ca2+ absorption from food. Intestine Ca2+ ions Bloodstream PTH Molecules Figure 16.12
Calcitonin • A peptide hormone produced by the parafollicular, or C cells • Lowers blood calcium levels • Antagonist to parathyroid hormone (PTH)
Calcitonin • Calcitonin targets the skeleton, where it: • Inhibits osteoclast activity (and thus bone resorption) and release of calcium from the bone matrix • Stimulates calcium uptake and incorporation into the bone matrix • Regulated by a humoral (calcium ion concentration in the blood) negative feedback mechanism