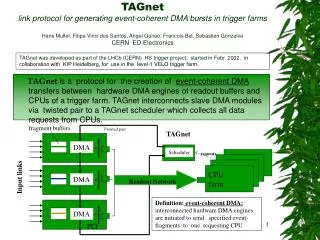
Outpatient PCI
Outpatient PCI. BCIS Autumn Meeting 2008 Stoke on Trent, United Kingdom Gerrit Jan Laarman, Department of Interventional Cardiology, OLVG, Amsterdam, The Netherlands Department of Interventional Cardiology, King’s College Hospital, London, United Kingdom. Outpatient PCI.

Outpatient PCI
E N D
Presentation Transcript
Outpatient PCI BCIS Autumn Meeting 2008 Stoke on Trent, United Kingdom Gerrit Jan Laarman, Department of Interventional Cardiology, OLVG, Amsterdam, The Netherlands Department of Interventional Cardiology, King’s College Hospital, London, United Kingdom BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI Definition of outpatient PCI = Discharge on the day of PCI BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI Why not? Possible reasons: • Medical • Legal • Financial • Psycho-social/cultural • Other (conservatism, egoism, laziness, stubbornness) BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI Medical reasons: • Cardiac complications • Acute stentthrombosis • Arrhythmia • Vascular complications • Access site bleedings • Other vascular complications • Other complications BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI There is no medical need to keep the patient overnight with an optimal result following elective TRI in well selected patients, meaning: • NO BLEEDING COMPLICATIONS • NO CARDIAC COMPLICATIONS BETWEEN 6-24 HOURS after PCI • Laarman et al. A pilot study of coronary angioplasty in outpatients. Br Heart J. 1994;72:12-5. • Kiemeneij et al. Transradial Palmaz-Schatz coronary stenting on an outpatient basis: results of a prospective pilot study.J Invasive Cardiol. 1995;7:5A-11A. • Kiemeneij et al. Outpatient coronary stent implantation. JACC 1997;29:323-7 • Slagboom et al. Actual outpatient PTCA: results of the OUTCLAS pilot study. CCI 2001;53:204-8. • Ziakas et al. Safety of same day discharge radial PCI. Am Heart J 2003;146:699-704. • Slagboom et al. Outpatient coronary angioplasty: feasible and safe. CCI 2005;64:421-7. BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI Legal reasons: • Efficacy and safety of outpatient PCI has been clearly demonstrated and described in a large series of publications from different groups in the past 15 years. • In several countries outpatient PCI has become clinical routine. • Thus, there is no ground for any legal objections anymore BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI Psycho-social/cultural reasons: • Dependent patients • Elderly patients • Insecure patients • Preference for staying overnight Keep those patients overnight! BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI Financial reasons: Macro-economic view Outpatient PCI using the transradial approach leads to a reduction in costs: • Shorter hospital stay • Shorter procedures • Less material consumption • Less bleeding complications • More efficient nursing care • Cheaper transportation (no ambulances between hospitals) • Back to work earlier BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI But: Micro-economic view In the Netherlands reimbursement for daycare PCI is € 5.500,= and for clinical PCI € 8.500,= BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI Other reasons: • “I don’t like changes” • “I don’t trust myself and like to sleep soundly” • “they’re cowboys” • “secundary prevention less effective after easy cases” • “they’re banalising PCI” • “I don’t do TRI because during PCI’s I’m always thinking about future CABG’s with the radial artery as a conduit” BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI: Rationale • All the advantages of TRI • Patient comfort • Beds available for sicker patients • Safe • Logistics: OLVG 36 cardiology beds/2400 PCI’s • Increases turn-over • Reduces waiting lists • Cost-effective BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI TRI • From alternative to preferred access site • Easy hemostasis (superficial course) • Less bleeding complications • No important nerve or vein near by • Allows ambulant/outpatient PCI • Patient preference • Cost-effective BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI TRI especially beneficial in • Elderly patients • Obese patients • Patients with musculo-skeletal disorders • Restless patients • Patients with severe peripheral artery disease • Patients with ACS requiring triple antithrombotic medication Now they can be treated as outpatients as well! BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI Requirements for outpatient PCI • Transradial approach • Dedicated infrastructure (lounge) • Dedicated and trained nursing and medical staff • Optimal information before and after PCI • Triage criteria BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI: Criteria • Good result elective PCI • No complications during PCI • Clinically stable • Uneventful course during 4-6 hours observation • Cardiac • Vascular • No other medical reasons to keep the patient hospitalized (e.g. renal failure) • Suitable psyco-social circumstances BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI: Current policy After >15 years experience (1992-2008) • Elective PCI • ± 60-80% in day care • UAP [clinical] • Same or next day (IIB-IIIA blockers) discharge • Inter-hospital: ± 100% transfer same day • Primary PCI: • Day 3 discharge • Interhospital: ± 100% transfer same day BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI:Lounge Day Care Cardiology • Atypical chestpain (120: 48 pts for further observation on ward) • Bleeding complications (120 minor bleeds;90 same day discharge): 30 pts for further observation on ward) • Angina without ECG-changes (75: 24 pts for further observation on ward/CCU) • Angina with ECG-changes (18 → CCU) • Acute stent thrombosis (2→ cath.lab.) • Coronary perforation (3 → CCU) • VF in lounge (1→ CCU) • No serious complications reported after discharge BCIS Autumn Meeting 2008, Stoke on Trent, UK
Elective PCI in elderly patients BCIS Autumn Meeting 2008, Stoke on Trent, UK
Elective PCI in elderly patients BCIS Autumn Meeting 2008, Stoke on Trent, UK
Elective PCI in elderly patients BCIS Autumn Meeting 2008, Stoke on Trent, UK
Elective PCI in elderly patients BCIS Autumn Meeting 2008, Stoke on Trent, UK
Outpatient PCI: Conclusion • TRI allows you to re-design the process of hospitalization of PCI patients • This lounge-like environment for ambulant and independent patients is the most extreme logistic manifestation of the transradial approach • This is the leanest, most efficient and most patient-friendly way of working • Insurance companies should be motivated to reward physicians following this approach instead of (financially) frustratingthem BCIS Autumn Meeting 2008, Stoke on Trent, UK