Download
1 / 48
500 likes | 865 Vues
High-Intensity Focused Ultrasound for Hepatocellular Carcinoma. Joint Hospital Surgical Grand Round Queen Mary Hospital 19/10/2013. Background. How HIFU works Indications / Contraindications Complications Current results. Hepatocellular carcinoma. Most common primary liver cancer

E N D
High-Intensity Focused Ultrasound for Hepatocellular Carcinoma Joint Hospital Surgical Grand Round Queen Mary Hospital 19/10/2013
Background How HIFU works Indications / Contraindications Complications Current results
Hepatocellular carcinoma • Most common primary liver cancer • Only 15% resectable disease on presentation • Inadequate liver function • Multifocality • Local ablative therapies for unresectable disease
Local ablative therapy • Radiofrequency ablation • Ethanol injection • Microwave ablation • High-intensity focused ultrasound
Background How HIFU works Indications / Contraindications Complications Current results
High-Intensity Focused Ultrasound • Focused ultrasound energy (0.8MHz) from distant transducer • Hyperthermia • Coagulative necrosis • Intact tissues in between
Animal studies in 1940s • Intended for treatment of Parkinson disease
Current clinical applications 1990s: Transrectal HIFU for prostate cancer 2000s: MRI guided HIFU for uterine fibroid Under investigation: Pancreatic tumour, bone tumours etc.
Ultrasound guided HIFU system Therapeutic ultrasound transducer Water tank Diagnostic ultrasound probe
Procedure • General anaesthesia • Immobilization • Interval cessation of ventilation • Prone / right lateral position
Procedure • Planning with diagnostic ultrasound • Slice-by-slice ablation from deep to superficial region
Grayscale change Before ablation After ablation
Advantages / disadvantages • Advantages • No internal bleeding • No needle tract seeding • Less liver derangement • Disadvantages • Needs general anaesthesia • Lengthened procedure
Background How HIFU works Indications / contraindications Complications Current results
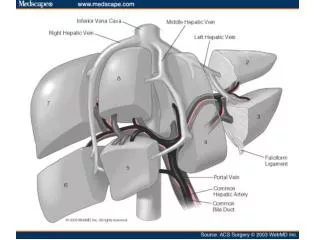
Indications • Small tumour • Less than 3cm: ablation rate >85% • Centrally located / liver dome tumour • Adjacent to major bile duct / veins • Child’s C liver function • Gross ascites Cheung TT et al. HPB 2013
Indications • Small tumour • Less than 3cm: ablation rate >85% • Centrally located / liver dome tumour • Adjacent to major bile duct / veins • Child’s C liver function • Gross ascites
Contraindications • Not fit for general anaesthesia • Cannot assume treatment position • Very poor liver function • Lesion not visualized by USG • Overlying hollow viscus • Deep tumour • Tumour close to overlying rib
Tumour close to rib Pre-ablation Post-ablation
Background How HIFU works Indications / Contraindications Complications Current results
Complications (10-20%) Skin burn Bruising • Pneumothorax • Incomplete ablation (10% for small tumours)
Background How HIFU works Indications / Contraindications Complications Current results
Unresectable HCC (n=49) • Child’s A (n=41) and B (n=8) cirrhosis • Median size 2.2cm (0.9-8cm) Ng KK et al. Annals of Surgery 2011
Unresectable HCC • Ablation rate 79.5% (n=39) • Risk factor: median tumour size (2.3cm vs. 3.8cm; p=0.03) Ng KK et al. Annals of Surgery 2011
HIFU v.s. RFA Small HCC
Small (<3cm) unresectable HCC (n=106) • Percutaneous RFA if feasible (n=59) • HIFU (n=47) if • Technically difficult percutaneous RFA • Liver dome tumour • Ascites • Child’s B cirrhosis Cheung TT et al. HPB 2013
HIFU vs. RFA Cheung TT et al. HPB 2013
Survival 81% 80% 34% 26% Cheung TT et al. HPB 2013
Liver tumours (n=30) and pancreatic tumours (n=6) • Tumour <1cm from • IVC / hepatic /portal veins (n=27) • Bile ducts (n=4) • 1 portal vein thrombosis (Pancreatic cancer) • No bile duct injury Franco O et al. AJR 2013; 195
HCC (n=39) with close proximity to major veins • No venous thrombosis / bile duct injury Zhang L et al. Eur Radiol 2008
Special condition Locally advanced HCC
Locally advanced (4-14cm, mean 10.5cm) HCC (n=50) • Randomized controlled trial • TACE + HIFU (n=24) • TACE only (n=26) Wu F et al. Radiology 2005
TACE + HIFU vs. TACE Wu F et al. Radiology 2005
Survival TACE + HIFU TACE only Wu F et al. Radiology 2005
Locally advanced HCC • Combined HIFU / TACE is a promising approach • On-going trial in QMH Wu F et al. Radiology 2005
Special condition Bridging to transplant
Retrospective study • Transplant candidates for HCC (n=49) • Bridging HIFU (n=5) • Bridging TACE (n=29) • No bridging therapy (n=15) • Non-transplant candidates with HIFU (n=5) Cheung TT et al. WJG 2013
Bridging to transplant Cheung TT et al. WJG 2013
Bridging to transplant • 3 patients in HIFU group received liver transplant • Pathology • Complete necrosis (n=2) • 90% necrosis (n=1) Cheung TT et al. WJG 2013
Liver transplant candidate • Effective bridging therapy to liver transplant Cheung TT et al. WJG 2013
Summary • Current applications • Ablative therapy for small unresectable HCC • Child’s C liver function • Tumour close to major pedicle • Combined with TACE for large HCC • Bridging therapy to liver transplantation • Under investigation • More clinical studies warranted