Download
1 / 20
200 likes | 423 Vues
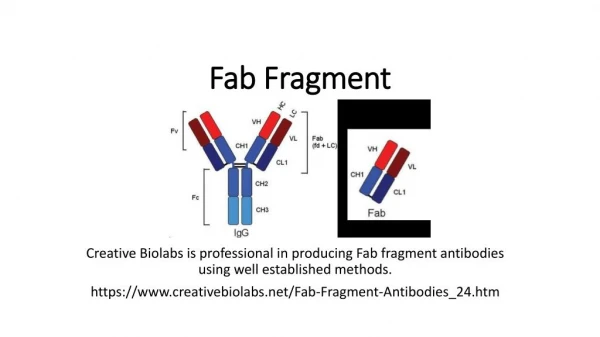
Ranibizumab Recombinant, humanized, monoclonal antibody antigen binding fragment (Fab) Neutralizes all known active forms of vascular endothelial growth factor-A (VEGF-A)

E N D
Ranibizumab • Recombinant, humanized, monoclonal antibody antigen binding fragment (Fab) • Neutralizes all known active forms of vascular endothelial growth factor-A (VEGF-A) • First drug shown to improve average vision in choroidal neovascular membrane (CNV) due to age related macular degeneration (AMD)# #Source: ANCHOR Trial
To determine whether a less frequent dosing of ranibizumab would also prevent vision loss in AMD related subfoveal CNV.
Best corrected visual acuity between 20/40 to 20/320. • Total CNV area (occult + classic) >50% of total lesion area. • Total lesion area <12 disc area (DA) in size. • Minimally classic or occult CNV with: • Loss of >1 Snellen’s line during last 6 months. • More than 10% increase in size on FA during last 6 months. • Subretinal haemorrhage in last 1 month.
Prior PDT, TTT, EBRT, subfoveal laser. • Permanent structural damage to central fovea. • Foveal subretinal haemorrhage >1 DA or >50% lesion area. • Prior anti-VEGF treatment.
Ranibizumab group: Monthly for 3 doses; quarterly thereafter • Sixty subjects :- 0.3 mg • Sixty one subjects :- 0.5 mg • Sham treatment group: • Sixty three subjects :- sham injections • Primary endpoint: • Mean change in visual acuity score. • Key secondary endpoints: • Proportion of subjects gaining/loosing 15 letters or more. • Mean change in area of CNV and area of leakage.
Sham treated group • Loss of 16.3 letters • Ranibizumab 0.3 mg • Loss of 1.6 letters • Ranibizumab 0.5 mg • Loss of 0.2 letters
Sham treated group • Loss of <15 letters in 49.2% • Ranibizumab 0.3 mg • Loss of <15 letters in 83.3% • Ranibizumab 0.5 mg • Loss of <15 letters in 90.2%
Sham treated group • Gain of >15 letters in 9.5% • Ranibizumab 0.3 mg • Gain of >15 letters in 11.7% • Ranibizumab 0.5 mg • Gain of >15 letters in 13.1%
Sham treated group • Increase in leakage area • Ranibizumab 0.3 mg • Decrease in leakage area • Ranibizumab 0.5 mg • Decrease in leakage area
Both ranibizumab groups maintained baseline visual acuity at the end of 12 months. • Gain in visual acuity score was maximum in first 3 months. • Decline in visual acuity score to baseline with quarterly dosing. • Significantly greater number of ranibizumab group subjects lost less than 15 letters. • No significant benefit in number of subjects gaining 15 letters or more.
Larger sample size with monthly injections and 2 years follow up results. • At 24 months, 90% subjects treated with ranibizumab had stable vision compared to 53% in sham-treated group. (p<0.001) • Improvement of at least 15 letters or more in 34% subjects receiving 0.5mg ranibizumab. (p<0.001)
Larger sample size with monthly injections. • With 0.5mg ranibizumab 96% subjects had stable vision compared to 64% in verteporfin PDT group. (p<0.001) • Improvement of at least 15 letters or more in 40% subjects receiving 0.5mg ranibizumab compared to 6% in verteporfin PDT group. (p<0.001)
The 3-month results from PIER mirrored MARINA and ANCHOR; however, visual acuity gains declined once quarterly dosing began. Quarterly injections of ranibizumab might be less effective than monthly dosing.# #Source: Genentech Press Release. Preliminary Results from a Phase IIIb Study Showed Patients with Wet AMD Treated with Lucentis Quarterly Experienced a 16-Letter Benefit over the Control Group at One Year.
PIER study suggests that decline in visual acuity was due to increase in vascular leakage and mean retinal thickness. OCT data were lacking at 4, 6, 7, 9 and 10 months precluding any assessment of temporal association between quarterly dosing and increase in mean retinal thickness.
OCT based, uncontrolled, variable dosing, single centre study. • Monthly injections for three months. • Further monthly injections during first year: • Increase in central retinal thickness of more than 100 micron • Loss of five or more letters. • Injections during second year: • Qualitative increase in amount of fluid on OCT.
Mean visual acuity improved by 11.1 letters • Forty three percent subjects gained 15 letters or more. • Average of 9.9 injections were given in 24 months. • OCT guided variable dosing regimen lead to comparable results but with fewer injections.# # Source: Am J Ophthalmol. 2009; 148: 43-58.e1.
PIER regimen of intravitreal ranibizumab for CNV due to AMD provides less benefit in visual acuity than continued monthly dosing. • Monthly or variable dosing may be needed in some patients to achieve maximum benefit of ranibizumab.
Comparison of Age-Related Macular Degeneration Treatment Trials (CATT) Vascular Endothelial Growth Factor (VEGF) Trap-Eye: Investigation of Efficacy and Safety in Wet Age-Related Macular Degeneration (AMD) (VIEW 2)