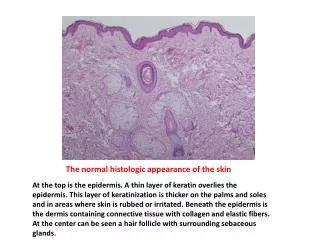
Download
1 / 20
210 likes | 245 Vues
Explore the significance of C4d staining in ABO-incompatible renal allografts and its prognostic implications without histologic lesions. Learn how C4d is a marker of humoral response detectable by immunofluorescence or immunohistochemistry.

E N D
The Significance of C4d Staining with Minimal Histologic Abnormalities Mark Haas Department of Pathology Cedars-Sinai Medical Center Los Angeles, California, USA
Outline/Objectives 1. To appreciate differences in the interpretation of positive C4d staining in ABO-incompatible renal allografts versus conventional and positive cross-match (HLA-incompatible) renal allografts 2. To review potential prognostic implications of C4d staining without histologic lesions of antibody-mediated or cellular rejection in ABO-incompatible versus conventional and positive cross-match renal allografts
C4d • Degradation product of complement factor C4, a component of the classical complement pathway that is typically initiated by antibody bound to antigen • After cleavage of remaining C4 domains, C4d remains covalently bound at site of C4 activation • Thus, C4d is a relatively long-lived marker of a humoral response • Easily detected in tissue sections by immunofluorescence or immunohistochemistry
C4d Staining in Renal Allografts: correlation with donor-specific Ab • Collins et al, JASN 10: 2208-14, 1999 100% of AR with +DSA were C4d+ No C4d in DSA- AR, CSA toxicity • Crespo et al, Transplantation 71: 652-8 2001 18/19 with steroid-resistant AR and DSA C4d+ 2/32 with steroid-resistant AR and no DSA C4d+ C4d positivity 95% sensitive for presence of DSA (IF) • Maueyyedi et al, JASN 13: 779-787, 2002 30% of early AR C4d+ - 90% had anti-donor antibody 2 morphologic subtypes of AMR - capillary, arterial Arterial had worse outcome • Bohmig et al, JASN 13: 1091-9, 2002 21/24 C4d+ cases had DSA by flow cytometric XM 50% of C4d- biopsies had DSA 93% specificity, 31% sensitivity (IHC on paraffin sections)
DiagnosticCriteriaforAcuteAMRinRenalAllograftBiopsies(L.C. Racusen et al, Am J Transplant 3: 1-7, 2003) • Morphologic evidence • Neutrophils and/or monocytes/macrophages in PTC and/or glomeruli (acute glomerulitis) • Arterial fibrinoid necrosis • Thrombi in glomerular capillaries, arterioles, and/or small arteries • Acute tubular injury (?) 2. Immunohistologic evidence • C4d in PTC • Immunoglobulin and/or complement in arterial fibrinoid necrosis • Serologic evidence • Circulating antibodies to donor HLA or other specific anti-donor antibodies at the time of biopsy
No TG TG Cosio et al, AJT 8:492-6,2008
What is the effect of C4d staining without histologic evidence of AMR in ABO-I grafts? 44 recipients of ABO-I grafts 1/00 – 6/07 37 met the following criteria: • One or more protocol biopsies were done during the first ~3 months post-transplantation, meeting Banff ’97 adequacy criteria • One or more subsequent protocol biopsies were done at 6 and/or 12 months post-transplantation, meeting the same adequacy criteria • C4d staining was done on all protocol biopsies
What is the effect of C4d staining without histologic evidence of AMR in ABO-I grafts? Of these 37 patients: 21 (Group A) had an initial (1 or 3 month) protocol biopsy meeting all of the following criteria: • >1+ diffuse PTC C4d • No ACR (Banff ’97 1a or greater) or histologic evidence of AMR (PTC neutrophil or mononuclear WBC margination [ptc >0], glomerulitis [g>1], TMA, or arterial/arteriolar fibrinoid change) • Presence of circulating antibody against donor blood group antigen(s) Of remaining 16 patients,12 had negative or focal and weak (<1+) PTC C4d on their initial protocol biopsy (Group B), while the other 4 had >1+ diffuse C4d but with PTC WBC margination (SC AMR; omitted). All had circulating anti-blood group antibody. No patient had anti-HLA Class I or Class II antibodies.
Dickenmann et al, Clin Nephrol 65: 173-179, 2006 • Examined outcomes in 22 patients having for-cause biopsies of conventional renal allografts that showed focal (n = 21) or diffuse (n = 1) peritubular capillary C4d staining by IF, no morphologic evidence of AMR or ACR, and no prior C4d+ biopsy. • 5/22 patients received anti-rejection therapy following the biopsy, while 17/22 continued to receive only baseline immunosuppression
+CM 3 month protocol bx SCr 1.0 mg/dl 2 + diffuse C4d, ptc 3 No ACR
Conclusions • Although based on a retrospective analysis of a relatively small number of patients, our findings suggest that diffuse PTC C4d deposition and circulating anti-blood group antibodies in the absence of clinical or histologic evidence of AMR is most likely associated with a decreased risk of scarring in ABO-incompatible renalallograftsin the relatively short term. • It will be important to determine if this apparent beneficial effect persists over the long term and in larger cohorts of patients from different centers. If true, this would indicate that C4d staining without other evidence of AMR in ABO-incompatible grafts most likely represents a state of stable accommodation.
Conclusions (continued) 3. Unlike the case in ABO-incompatible grafts, in positive crossmatch (and conventional) renal allografts C4d deposition in the absence of histologic evidence of AMR appears to be uncommon, and may in fact indicate (potentially reversible) graft injury. However, there may be notable exceptions.
Department of Surgery Robert Montgomery Dorry Segev Daniel Warren Chris Simpkins Diane Lepley Jayme Locke Department of Pathology Lorraine Racusen Serena Bagnasco Karen King Department of Medicine Edward Kraus Hamid Rabb Andrea Zachary Hafiz Rahman