Download
1 / 20
210 likes | 297 Vues
Learn about the triggers and pathogenesis of urticaria, diagnostic tests, associated conditions, and pharmacologic treatment options for chronic urticaria. Explore the manifestations of atopic dermatitis and its immune responses. Discover testing methods to identify specific triggers.

E N D
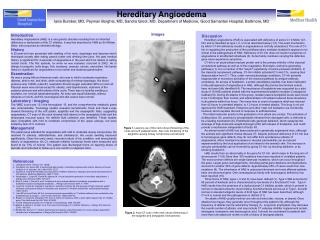
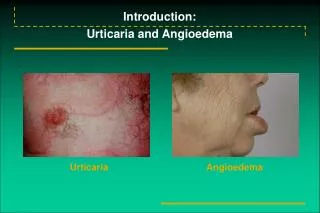
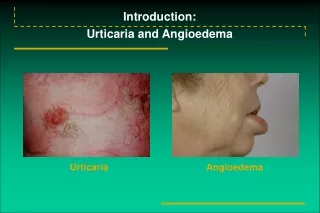
Introduction:Urticaria and Angioedema • Urticaria • Angioedema
Etiology of Urticarial Reactions:Allergic Triggers • Acute Urticaria • Drugs • Foods • Food additives • Viral infections • hepatitis A, B, C • Epstein-Barr virus • Insect bites and stings • Contactants and inhalants (includes animal dander and latex) • Chronic Urticaria • Physical factors • cold • heat • dermatographic • pressure • solar • Idiopathic
Role of Mast Cells in Chronic Urticaria:Lower Threshold for Histamine Release • Release threshold decreased by: • Cytokines & chemokines in the cutaneous microenvironment • Antigen exposure • Histamine-releasing factor • Autoantibody • Psychological factors Cutaneous mass cell • Release threshold increased by: • Corticosteroids • Antihistamines • Cromolyn (in vitro)
An Autoimmune Basis for Chronic Idiopathic Urticaria: Antibodies to IgE
Initial Workup of Urticaria • Patient history • Sinusitis • Arthritis • Thyroid disease • Cutaneous fungal infections • Urinary tract symptoms • Upper respiratory tract infection (particularly important in children) • Travel history (parasitic infection) • Sore throat • Epstein-Barr virus, infectious mononucleosis • Insect stings • Foods • Recent transfusions with blood products (hepatitis) • Recent initiation of drugs • Physical exam • Skin • Eyes • Ears • Throat • Lymph nodes • Feet • Lungs • Joints • Abdomen
Laboratory Assessment for Chronic Urticaria • Possible tests for selected patients • Stool examination for ova and parasites • Blood chemistry profile • Antinuclear antibody titer (ANA) • Hepatitis B and C • Skin tests for IgE-mediated reactions • Initial tests • CBC with differential • Erythrocyte sedimentation rate • Urinalysis • RAST for specific IgE • Complement studies: CH50 • Cryoproteins • Thyroid microsomal antibody • Antithyroglobulin • Thyroid stimulating hormone (TSH)
Histopathology • Group 2: • Polymorphous perivascular infiltrate • Neutrophils • Eosinophils • Mononuclear cells • Group 3: • Sparse perivascular lymphocytes
Urticaria Associated With Other Conditions • Collagen vascular disease (eg, systemic lupus erythematosus) • Complement deficiency, viral infections (including hepatitis B and C), serum sickness, and allergic drug eruptions • Chronic tinea pedis • Pruritic urticarial papules and plaques of pregnancy (PUPPP) • Schnitzler’s syndrome
H1-Receptor Antagonists: Pros and Cons for Urticaria and Angioedema • First-generation antihistamines (diphenhydramine and hydroxyzine) • Advantages: Rapid onset of action, relatively inexpensive • Disadvantages: Sedating, anticholinergic • Second-generation antihistamines (astemizole, cetirizine, fexofenadine, loratadine) • Advantages: No sedation (except cetirizine); no adverse anticholinergic effects; bid and qd dosing • Disadvantages: Prolongation of QT interval; ventricular tachycardia (astemizole only) in a patient subgroup
Four-week Treatment Period:Fexofenadine HCl Mean Pruritus Scores/Mean Number of Wheals/Mean Total Symptom Scores
Treatment of Urticaria: Pharmacologic Options • Antihistamines, others • First-generation H1 • Second-generation H1 • Antihistamine/decongestant combinations • Tricyclic antidepressants (eg, doxepin) • Combined H1 and H2 agents • Beta-adrenergic agonists • Epinephrine for acute urticaria (rapid but short-lived response) • Terbutaline • Corticosteroids • Severe acute urticaria • avoid long-term use • use alternate-day regimen when possible • Avoid in chronic urticaria (lowest dose plus antihistamines might be necessary) • Miscellaneous • PUVA • Hydroxychloroquine • Thyroxine
Atopic Dermatitis: Acute, Subacute, and Chronic Lesions • Acute Cutaneous Lesions • Erythematous, intensely pruritic papules and vesicles • Confined to areas of predilection • cheeks in infants • antecubital • popliteal • Subacute Cutaneous Lesions • Erythema excoriation, scaling • Bleeding and oozing lesions • Chronic Lesions • Excoriations with crusting • Thickened lichenified lesions • Postinflammatory hyperpigmentation • Nodular prurigo
Immune Response in Atopic Dermatitis • Markedly elevated serum IgE levels • Peripheral blood eosinophilia • Highly complex inflammatory responses > IgE-dependent immediate hypersensitivity • Multifunctional role of IgE (beyond mediation of specific mast cell or basophil degranulation) • Cell types that express IgE on surface • monocyte/macrophages • Langerhans’ cells • mast cells • basophils
Atopic Dermatitis:Tests to Identify Specific Triggers • Skin prick testing for specific environmental and/or food allergens • RAST, ELISA, etc, to identify serum IgE directed to specific allergens in patients with extensive cutaneous involvement • Tzanck smear for herpes simplex • KOH preparation for dermatophytosis • Gram’s stain for bacterial infections • Culture for antibiotic sensitivity for staphylococcal infection; supplement with bacterial cultures • Cultures to support tests bacterial, viral, or fungal
Topical Corticosteroids • Ranked from high to low potency in 7 classes • Group 1 (most potent): betamethasone dipropionate 0.05% • Group 4 (intermediate potency): hydrocortisone valerate 0.2% • Group 7 (least potent): hydrocortisone hydrochloride 1% • Local side effects: Development of striae and atrophy of the skin, perioral dermatitis, rosacea • Systemic effects: Depend on potency, site of application, occlusiveness, percentage of body covered, length of use • May cause adrenal suppression in infants and small children if used long term
Antihistamines and Other Treatments • Standard Treatment • Oral antihistamines to relieve itching • Moisturizer to minimize dry skin • Topical corticosteroids • Hard-to-manage Disease • Antibiotics • Coal tar preparations (antipruritic and anti-inflammatory) • Wet dressings and occlusion • Systemic corticosteroids • UV light therapy • Hospitalization