Download
1 / 38
390 likes | 559 Vues
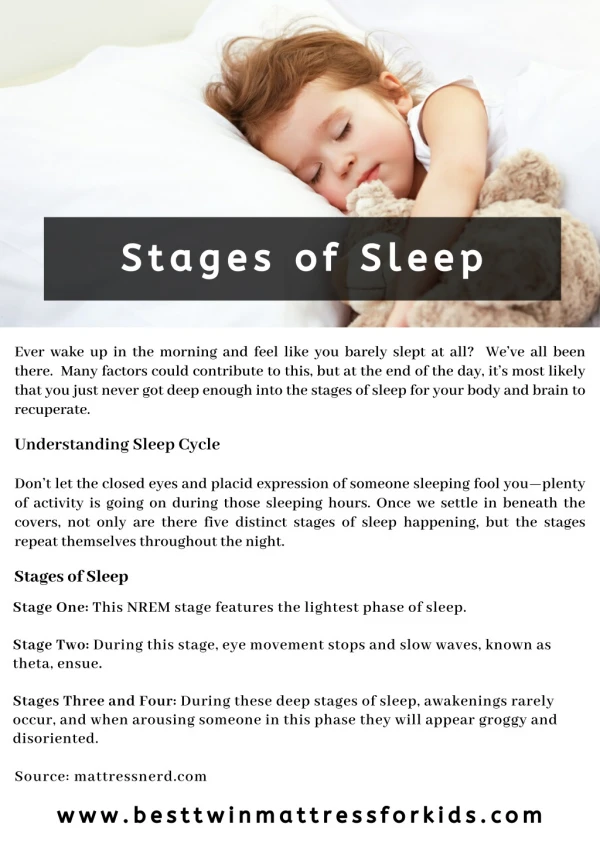
The nature of Sleep: an Ultradian Rhythm Rhythms of a length shorter than <24 hours (which can occur more often in a 24 hour period). Aims To know the nature of sleep To understand the difference between the stages of sleep To be able to explain the various stages of sleep. Key concepts .

E N D
The nature of Sleep: an Ultradian RhythmRhythms of a length shorter than <24 hours (which can occur more often in a 24 hour period) Aims To know the nature of sleep To understand the difference between the stages of sleep To be able to explain the various stages of sleep
Key concepts • Ultradian • 5 cycles • 90 mins • Sleep escalator • Alpha • Theta • Delta • Delta • Beta
Revision of concepts • Ultradian rhythms • Sleep stages • Measuring sleep • EEG, EMG, EOG • Sleep deprivation studies • RG, PT, Haingoc, Maureen • Lifespan changes • Clock genes • Evaluation • Objective evidence • Artificiality of sleep laboratory • Individual differences • Under researched groups • Motivated participants • Reductionist definition • Explanations • Restoration • Evolutionary
Examiner report 2012 • Question 01 • Responses to this short answer question were often disappointing. The focus needed to be on ultradian rhythms, but many students were diverted into describing the stages of REM and NREM sleep in far too much detail. For full marks the focus needed to be on the patterning of the stages and the fact that the ‘sleep staircase’ repeats throughout the night in a rhythmic pattern. • Many answers failed to identify an ultradian rhythm, confusing ultradian with infradian. It is also worth noting that body temperature is not an ultradian rhythm. It is a circadian rhythm, with one peak and one trough every 24 hours.
What happens in the brain? • One of the most important centres is the reticular activating system (RAS), which is located in the brainstem region. • A key component of the RAS is a group of cholinergic nuclei near the pons -midbrain junction. • Many of the neurons in these nuclei are highly active during waking and REM sleep, and inactive during non-REM sleep. • Acetylcholine, noradrenaline, serotonin and glutamate are involved in the regulation of the sleep and wake states. • sleep disorders may arise from abnormalities in the areas of the brain and the neurotransmitters involved in the control of sleep.
ALPHA THETA DELTA DELTA BETA S1 A S2 T S3 D S4D S5 B REM Repairing the Brain GH Repairing the body
imp. For psy. As a science How sleep is measured: Operationalising sleep (quantitatively) • Electroencephalographs (EEGs) measure electrical activity or brain waves, • EEG readings show frequency and amplitude which indicate activity, they differ depending on the stage of sleep. The stages and activity vary from cycle to cycle. • Electro-oculograms (EOGs) measure eye movement • Electromyograms (EMGs) measure muscle movement and have been used to distinguish the stages and cycles of sleep.
Sleep • The use of EEGs (electroencephalography) has made the investigation of dreaming possible. In using EEGs , electrodes are attached to the scalp to measure the gross electrical activity of the brain and allow researchers to classify different levels of arousal. • EEG produces brain waves that vary in terms of frequency and amplitude (the number of waves per second and the height of the waves respectively). Frequency is measured in Hertz (Hz) which consists of the number of waves per second. • Sleep has been divided into 2 main classes: SWS – slow wave sleep, and REM- Rapid eye movement sleep (paradoxical sleep) • Further investigation led to SWS being sub-divided into 4 stages
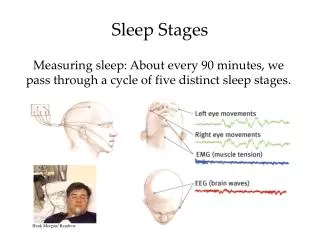
Stages of Sleep: An UltradianRhythm ATDDB • Stage 1 • Relaxation with synchronous brain waves - A • Stage 2 • EEG becomes slower and larger - T • Stage 3 • EEG consists of long, slow delta waves -D • Stage 4 • Slow-wave sleep (SWS) - D • Stage 5 REM • Rapid eye movement or REM sleep - B Non-REM/sws REM 90 mins cycle; 5 cycles a night
Cyclic variations in EEG during sleep and their relation to eye movements, body motility, and dreaming
Sleep escalator/Staircase • 1, 2, 3, 4, 3, 2, REM • 2, 3, 4, REM • 2, REM • 2, REM • 2, REM • NonREM/SWS 3/4 decreases as the night progresses • REM length increases as the night progresses • 10min, 10min, 40min, 60mins+
REM Sleep and Dreaming • Aserinsky and Kleitman (1955) • First discovered the association between REM sleep and dreaming • Dement and Kleitman (1957) • Between 70% and 75% of participants woken in REM sleep report dreaming • Green (1994) • 30% of sleepers in SWS report dreaming • REM dreams • Are vivid and detailed • Non-REM dreams • Are vague and less coherent
Stages 1-4 are often seen as deeper levels of sleep. The deeper you go the more difficult it becomes to wake someone up. REM sleep is known as paradoxical sleep (the brain is awake and the body is paralysed). A feature of REM sleep is the eyeballs move rapidly in the socket. Dreaming is often reported in REM sleep (less common in 1-4 and less vivid). REM dreaming usually include vivid visual imagery, sounds, smells etc., and also a story.
Contrasting characteristics of SWS and REM sleep • During SWS sleep, sensory information is inhibited from entering the consciousness by a lower brain area called the thalamus (evolutionary structure that controls the amount of sensory information that reaches higher brain areas, T-cells are produced here). This may also serve to maintain sleep by stopping distractions. Also, there is a move to conserve heart rate, blood pressure and respiratory rate decreases.
REM/PL • During REM sleep motor regions of the cortex are activated. Despite this activation, the motor neurones (that control skeletal muscles) are normally inhibited (see sleep disorders). Therefore the instructions to move are countermanded by other brain areas, leading to temporary paralysis. Unlike SWS some sensory information enter from the external world and can be incorporated into dreams.
Sleep escalator • Up and down the “sleep escalator” • Most people have 5 cycles of sleep a night that last approximately 90 minutes. Slow-wave sleep (SWS) occurs in only the first two cycles; REM sleep occurs in all of the cycles, and increases during the course of the night’s sleep. • Traditionally, self-report data was used before the development of the recording technology
Five cycles of 90 mins • 1st cycle: • go down the sleep escalator from stage 1- 4; then ascend through stage 3 and then stage 2. REM sleep follows this and lasts 10 mins. • 2nd cycle: • begin at stage 2, for 20 mins, then descend through stage 3 to stage 4, lasts 30 mins. REM sleep for 10 mins. • 3rd cycle: • start at stage 2 for 1 hour, then REM sleep for 40 mins. • 4th cycle: • start at stage 2 for 70 mins, then REM sleep for 1 hour. • 5th cycle: • start at stage 2, followed by REM sleep. This is known as the emergent cycle as we may wake from either cycle. We are more likely to remember our dream if we wake during REM sleep.
Stage 1: Last approximately 15 minutes. The body relaxes and the individual feels drowsy. The EEG activity is characterised by alpha waves that have a frequency of 8-12 cycles per second (cps or Hz). • The EOG indicates slow rolling eye movements and the EMG shows reductions in muscle tension. Heart rate and temperature also fall. A hypnogogic state may occur during the transition from wakefulness to sleep in which hallucinations may be experienced, e.g. the feeling of falling. • As this is the lightest stage of sleep we are easily awakened and may feel as if we have been jolted awake.
Stage 2: Lasts approximately 20 minutes. The EEG activity is characterised by larger and slower theta waves (4-8Hz) and short bursts of high frequency sleep spindles (12-14Hz). • K-complexes also occur, which are our responses to external stimuli (e.g. noise) and internal stimuli. • The EOG shows little eye movement and the EMG shows the muscles are relaxed. It is still easy to be awakened
Stage 3: Lasts approximately 15 minutes. The EEG activity is characterised by long, slow delta waves (1-5Hz) with some sleep spindles. The EOG and EMG are the same as stage 2.
Stage 4: Lasts approximately 30 minutes. Stage 4 is also known as slow-wave sleep (SWS) because of the long, slow delta waves of the EEG. The EOG and EMG show very little activity. This is deep sleep and so it is hard to wake somebody from. • Other physiological activity includes body temperature, heart rate and blood pressure dropping to their lowest point and (GH) growth hormones are secreted. It is also the stage when sleepwalking, sleep- talking and “night-terrors” (a nightmare where the individual appears wide awake but is asleep) can occur.
Stage 5: Lasts approximately 10 minutes in the 1st cycle and builds up to an hour by the 4th and 5th cycles. The EEG activity is characterised by beta waves (13-30Hz), which also occur during a relaxed waking state and this high level of brain activity is linked to dreaming. This stage is also known as REM sleep because of the rapid eye movements and has also been called paradoxical sleep because the EEG readings show that the brain is very active, whilst the EMG readings show that the body is paralysed. Consequently it is the hardest stage to wake somebody from. This paralysis is for a good reason because REM sleep is when most (but not all) dreaming occurs and so the paralysis prevents us from acting out our dreams.
Evaluation Objective evidence – EEG, EOG and EMG provide objective measures of sleep which means they are less subject to bias. Self-report is vulnerable to bias and distortion, due to researcher effects and participant reactivity, therefore it may lack validity. Weakness of the self-report method – The self-report method yields subjective data compared to the objective measurements of EEG, EOG and EMG. Artificialityof sleep laboratory- The sleep lab is an artificial condition and people are “wired up” to machines. The sleep lab is reductionist as it does not reflect many factors that can influence sleep in real life. The research lacks mundane realism and this means that the findings lack generalisability and ecological validity may be lacking. Universality : There are some universal characteristics of sleep as stages 3 and 4 occur only in the 1st two cycles and REM sleep always increases in duration with each successive cycle. Individual differences – Most people have 5 sleep cycles and sleep for around 8 hours. But many people sleep much less than this and much more. Patterns of sleep vary from each individual
Sleep Deprivation studies CBA To understand the consequences of sleep deprivation To be able to evaluate sleep research
Key concepts • Severe side effects (peter) • Mild side effects (RG) • Hallucinations • Cognitive disruption • IDA: Human Ethics • IDA: Animal ethics • Generalisation issues for Psychology as a science • Extrapolation from animal research studies CBA
ConsequencesMeta-analysis by Huber-Weidman (1976). • Huber-Weidman reviewed a large number of sleep deprivation studies and summarised the findings into common effects experienced over 6 nights of sleep deprivation. (Delusions) • The effects included feeling distress as a consequence of lack of sleep, a strong desire to sleep, periods of micro-sleep (a temporary loss of awareness experienced by sleep deprived people when awake), delusions, and, by the sixth night, “sleep deprivation psychosis”, which involves a sense of depersonalisation, loss of identity, and difficulty in coping with environmental demands and other people.
Research evidence sleep deprivation • Case Studies Peter Tripp, a New York DJ took part in a “wakeathon” for charity, where he stayed awake for 8 days. Severe The effects of this included delusions and hallucinations, e.g. he thought his desk drawer was on fire. Randy Gardner, a 17 year old student, stayed awake for 11 days and experienced mild symptoms effects included disorganised speech, blurred vision, and a small degree of paranoia, which was related to the effects of sleep deprivation as he felt people thought he was stupid due to his impaired functioning.
Restoration theory Peter Tripp instead of REM he hallucinated see video In 1977, Maureen Weston of the UK went without sleep for 449 hours (18.7 days). She began to hallucinate towards the end but reported no lasting effects from her rocking chair marathon. Without quantification it has no validity
The “rotating rats” study. • Rechtschafffen et al (1983), two rats were placed on a disc above a container of water, one was able to sleep but the other wasn’t - as when the EEG indicated sleep the disc began to rotate and so the rat fell into the water. • All of the sleep-deprived rats died within 33 days; the rats that were not sleep deprived appeared to suffer no ill effects as a result of the study. Ethics?
Jouvet (1967) • The “flower pot” technique. Jouvet (1967) used this to test the effect of REM sleep deprivation in cats. Cats were placed on a flowerpot in a tank of water. They were able to sleep without falling off during NREM but fell off as soon as they entered REM due to loss of muscle tone during the paralysis of REM sleep. • Continued REM deprivation proved fatal. Ethics?
The brain damaged patient. • Lugaressi et al (1986) reported the case of a man who, as a consequence of brain damage, could hardly sleep at all. He was unable to function normally and eventually died.
Fatal familial insomnia: Genetic Sleep normal until middle age then can not sleep, leading to death in 2 years. Autopsies have revealed a degeneration of the Thalamus, which may be the cause of the onset of insomnia. During SWS sleep, sensory information is inhibited from entering the consciousness by the thalamus (which controls the amount of sensory information that reaches). This may also serve to maintain sleep by stopping distractions. These are rare and the clear brain damage makes causality very difficult and also generalisation is difficult.
HW OpenHive • Complete sheet 1: Sleep • Complete sheet 2: sleep case studies • Complete a Sleep diary (bed/awake) for 7 days • Describe the nature of sleep (8 marks)
Describe the nature of sleep (8 marks) • Ultradian rhythms • Sleep stages • Sleep escalator • Measuring sleep • EEG, EMG, EOG • Sleep deprivation studies • RG, PT, Haingoc, Maureen • Lifespan changes