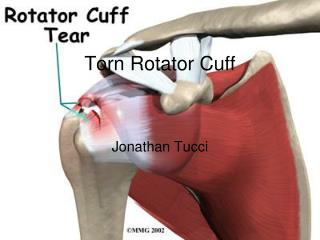
Rotator Cuff Tears
Rotator Cuff Tears. Reza Omid, M.D. Assistant Professor Orthopaedic Surgery Shoulder/Elbow Reconstruction & Sports Medicine Keck School of Medicine University of Southern California. Anatomy. Muscles? Innervation? Function?. Rotator Cuff Tears Natural History. ?.

Rotator Cuff Tears
E N D
Presentation Transcript
Rotator Cuff Tears Reza Omid, M.D. Assistant Professor Orthopaedic Surgery Shoulder/Elbow Reconstruction & Sports Medicine Keck School of Medicine University of Southern California
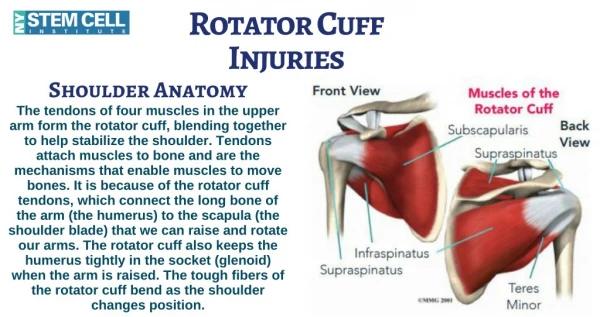
Anatomy • Muscles? • Innervation? • Function?
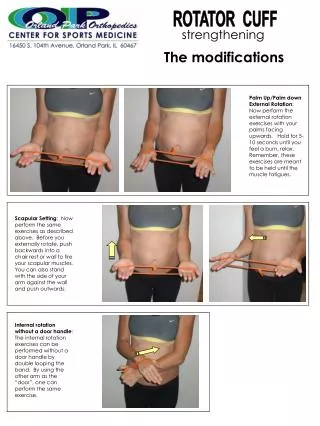
Rotator Cuff TearsTreatment • Not standardized • When do we maximize conservative care? • When is early surgical intervention appropriate?
Rotator Cuff Repair Surgical Indications • Variations in Orthopaedic Surgeon’s Perceptions about Indications for Rotator Cuff Surgery – Dunn, et al, JBJS ’05 • Sig variation • Lack of agreement • Surgical discussion • Role of PT • Prevent progression of tear
Asymptomatic TearWhy? • Mechanical Factors? • Force couples • Demographic Factors?
Proximal Humerus Migration • Why Does it Happen??
Rotator Cuff DisordersGlenohumeral Kinematics • Normal Cuff Head Centered • Tendinitis, Fatigue Superior Migration • Symptomatic RCT’s Superior Migration • Asymptomatic RCT’s ? Poppen & Walker, JBJS ‘75
Journal of Shoulder & Elbow Surgery • 2000;9:6-11
Results • Normals Ball & socket kinematics • Symptomatic RCT’s Superior head migration • Asymptomatic RCT’s Superior head migration (greater variability)
Conclusions • Loss of rotator cuff integrity (both symptomatic and asymptomatic) was associated with superior head migration • Superior head migration did not necessarily correlate with symptoms
Conclusions • Implies normal glenohumeral kinematics do not need to be restored with surgery
Journal of Bone and Joint Surgery, 99A, 2009
Bilateral Two-Tendon RCT • 30 Degree Abducted
Glenohumeral KinematicsAsympt vs Sympt RCT • Asymptomatic w/ less superior migration (smaller tears) • Both sympt/asympt superior in massive tears • Critical size for superior migration • 1.5 cm tear Jay Keener, JBJS 2009
Journal of Shoulder and Elbow Surgery 10:3, 2001
Methods • Shoulder Ultrasound employed at Washington University since 1984 (Unique Study Opportunity) • Routine bilateral exams • Predict large # of asymptomatic tears
ResultsSymptomatic Progression • 23/45 (51%) became symptomatic • avg 2.8 yrs from US
Conclusions • 39% total had tear size progression • No tears decreased in size (don’t heal on their own) • Relationship between symptoms and tear progression?
Journal of Bone and Joint Surgery 2006; 88-A, 1699-1704
Methods • Presence of unilateral shoulder pain (n=588) • Bilateral intact cuffs (n=212) • Unilateral tear* (n=191) • Bilateral tears* (n=185) • Demographic questionnaire data obtained for 586/588 • Age, tear size, side, thickness, family hx compared between symptomatic and asymptomatic individuals * tear: partial-thickness or full-thickness
Results • Correlation with Pain • Associated with dominant side (p<0.01) • 65% painful tears on dominant side • Associated with larger tears (p<0.01) • Symptomatic side 25% larger than asymptomatic • No other demographic feature significant
Results • Cuff disease increased with age • No tear – 48.7 yo • Unilateral tear – 58.7 yo • Bilateral tear – 67.8 • 50% likelihood of bilateral tear after age 66 yr if present with painful tear, (p<0.01)
Healing of RCR Influence of Age • Outcome/tear integrity of massive tears – JBJS 2004 • Tear integrity with double-row repair – AJSM 2009 • Outcome/ tear integrity of PTRCR – JBJS 2009 • Outcome/tear integrity of Revision RCR – JBJS 2010 Avg patient age healed: 55 yo Avg patient age not healed: 63 yo
Conclusions Demographics • Unilat tear in young • Bilat tear in older • Tears rare before 40 yo. • Tears common after 61 yo.
Conclusion • Intrinsic etiology for Cuff Disease • High incidence asympt./bilat disease • Increased tear size important for pain • High index of suspicion in high risk groups
Symptomatic Transition of Asymptomatic Rotator Cuff Tears Mall et al JBJS 2010
Conclusions • Over a 2 year period 21% of patients with an asymptomatic rotator cuff tear became symptomatic • Symptomatic transition of asymptomatic cuff tears is associated with significant increases in pain and loss of function • Tear size progression may play a significant role in symptomatic transition. • No significant changes seen in glenohumeral kinematics or shoulder strength upon symptomatic transition. (early detection is key!)
UltrasonographyAccuracy • Varies among institutions • 60% accuracy JBJS’86 • Not widely accepted
Journal of Bone and Joint Surgery 2000 • 82-A:498-504
Methods Validated accuracy • Teefey et al, JBJS ’04 • Compare to MRI • Pricket et al, JBJS ’03 • Post op shoulder • Teefey et al, JBJS ’00 • Compare to surgery • Middleton et al, JBJS ’86
Fatty Degeneration vs Fatty Infiltration • Galatz vs Gerber • What is the difference? • Why does it happen?
Degeneration vs Infiltration • Gerber: fatty cells infiltrate the muscle once the pennation angle changes • Galatz: fat cells develop from pluripotent cells found within the muscle itself, the process of infiltration does not occur
Fatty degeneration of the rotator cuff muscles Normal rotator cuff Fat-infiltrated infraspinatus
Fatty degeneration of the rotator cuff muscles Normal Supraspinatus Fat-infiltrated Supraspinatus Wall et al Accepted for pub JBJS 2012
What is atrophy? • Tangent Sign?
Methods • 262 pts from prospective cohort • Compare fatty degeneration to : • Tear location (relative to biceps) • Tear size ( number of muscles)
Results • 35% of full tears with sig fatty degeneration • Fatty degeneration in full-thickness tears only • Fatty degeneration highly correlated with proximity of tear to biceps
Conclusions • Disruption of anterior supraspinatus is strongly associated with development of fatty degeneration • Supports rotator cable concept for cuff (Burkhart): disruption of anterior cable is key!
Rotator Cuff Tears • Conventional concept: • Start from the anterior portion of supraspinatus insertion near the biceps tendon • Propagate posteriorly • Supraspinatus – almost always involved Codman EA, 1934; Keyes EL, 1933; Hijioka A, 1993; Matsen III FA, 1998; Lehman C, 1995
Superior Supraspinatus Infraspinatus Biceps tendon Posterior Anterior Teres Minor Humeral Head Subscapularis Inferior
Wash U Clinical Experience DT IS SS BT HH