Download
1 / 41
410 likes | 670 Vues
Rotator Cuff Arthropathy. Andre Le Leu Physiotherapy Clinical Specialist Shoulder and Elbow Unit Stanmore, UK. Contents. Anatomy Pathology Sub-acromial Impingement Syndrome Clinical Assessment Treatment methodology. Anatomy. Anatomy. Acromium. Rotator interval. Supraspinatus.

E N D
Rotator Cuff Arthropathy Andre Le Leu Physiotherapy Clinical Specialist Shoulder and Elbow Unit Stanmore, UK
Contents • Anatomy • Pathology • Sub-acromial Impingement Syndrome • Clinical Assessment • Treatment methodology
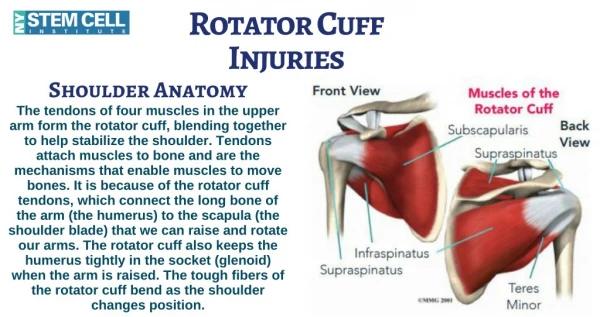
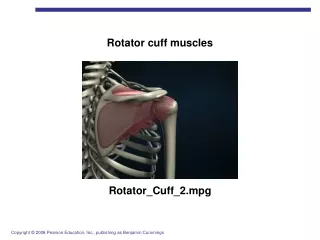
Anatomy Acromium Rotator interval Supraspinatus Posterior/ Superior Zone Infraspinatus Corocoid Anterior Zone Teres minor Subscapularis Glenoid NB: Subacromial Bursa not illustrated here but a critical element
Biomechanical Considerations Deltoid Suprasp. Infraspin Subscap Teres Minor
Cable Theory subscap Teres Minor Posterior Pillar Anterior Pillar LHBT Supra/infra sp.
Rotator Cuff Tendonopathy 40 yrs 50 yrs 60 yrs 80 yrs + Intra-substance tears Plasma enrichment Surgical debridement PHYSIOTHERAPY +++ Salvage ops Tendon transfers Constrained TSR FUNCTIONAL REHAB ‘Repetitive strain’ overuse Biomechanical impingement Angiogenesis Up regulation of fibroblast activity PHYSIOTHERAPY +++++++ Rotator cuff tears Rehab Surgery GENTLE PHYSIOTHERAPY
Rotator Cuff Examination • No test is absolute and definitive • Tests are merely a provocation symptoms rather than a confirmation of diagnosis (Lewis, 2008) • 90% of diagnoses are made from the patient history (Malone, 2005)
Examination • Look…. Postural alignment Bony landmarks Muscle bulk/atrophy General (scars, limb perfusion etc) • Feel…. Palpation (joint lines, muscle belly, ligaments/bursa) • Move…. Active movement, passive movement, resistance DO NOT FORGET NEUROVASULAR COMPONENTS / CLEARING TESTS
Special Tests • Supraspinatus • Jobes Test 90 degrees scaption Internal rotation (thumb down) Without resistance then with resistance Pain and or weakness Modification to start in thumbs up and run resistance testing through range to include rotator interval component. • Initiation of Abduction testing • Arm by the patients side • Palpate the Humeral Head • Assess resisted abduction • Weakness, pain, superior translation of humeral head • are all indicative of a positive test
Subscapularis • Gerber’s Lag sign As above but the therapist positions the hand ways from the spine and the patient must hold this position. (80% sensitivity for small tears) • Gerber’s lift off test Hand behind the back at 90 degrees elbow flexion The patient must keep the arm away from the spine The Therapist can add resistance (90% sensitivity for weakness or pain) • LaFosse belly press Hand rests on belly with wrist at neutral away from the forearm Held away from the body. The patient pulls the entire arm into the stomach (watch for drop of elbow or wrist), can also add therapist resistance to the outside of the elbow Good for patients with restrictions to movement Recruitment of P.major in 25% clouds the examination
Infraspinatus and Teres Minor • Resisted testing 1. External rot lag sign (ERLS) with arm at waist the therapist positions arm in full external rotation and the lets go while the patients attempts to hold this position. You can then add therapist resistance and required looking for pain/weakness. 2. Patient Holds arms in 60 degrees scaption with elbows at 90 degrees. Patient must resist internal rotation movement against the therapist. Pain and or weakness can be indicative of posterior cuff insufficency.
Infraspinatus and Teres Minor • Patte’s Test 90 degrees of abduction and external rotation, the patient must hold against resistance. Watch for correct scapulo-thoracic alignment Can test eccentric control element • Hornblowers Sign Arm held in 90 degrees scaption with hand in front of the mouth (supination). Patient must move the arm out into external rotation against gravity, however the therapist can also look to add resistance. • Hornblowers lag sign Arm is positioned at 90 degrees in scaption with full external rotation by the therapist. The Patient must the hold this position once the therapist lets the arm go. A positive drop sign is indicative of a massive posterior cuff tear.
Biceps tendon • Check for Popeye sign (rupture of LBHT) • Speeds test Patient holds straight arm in supination at 90 degrees flexion and tries to elevate the arm against the therapists resistance. Pain indicative of provocation. 90% Sensitivity and 15 % specificity (Malone 2005) • LaFosse AERS test(abduction, ext rot, supination) Arm is held at 90 degrees abduction and externally rotated with elbow at 90 degrees in pronation. The Therapist provides resistance as the patient supinates the arm Pain is indication of possible biceps irritation or SLAP tear • Yergason’s test • arm by side and elbow at 90 degrees, the therapist holds the patients hand and resists the patient moving into supination while palpating the LHBT. • Look for pain and or subluxation of tendon from bicepital groove
Shoulder Impingement Syndrome • Extrinsic Primary Acromial shape • ACJ pathology • Hypertrophied CA lig • Chronic Synovitis of Bursa • Secondary Instability (micro and gross) • Posterior capsule tightness • Neurogenic • S/T dysrythmia • Intrinsic Hypovascularity • Age related degenerative changes • Overuse • Cuff weakness/fatigue/cuff rupture
Impingement Tests • Neer’s Test • Therapist stands behind the patient and stabilizes the scapular. The holds the arm in ‘thumbs down’ in full elbow extension. • The maneuver is to the elevate the arm into f.flexion • Provocation of pain (80% specificity for bursa and cuff problems Malone et al) • Hawkins (Kennedy) Test • Therapist holds he arm in the plane of the scapular with the elbow at 90 degrees. • The hand is put into a thumbs down position and then the arm is medially rotated, a positive test provokes pain/restriction of movement (90% sensitivity, Malone et al)
Acromioclavicular joint • Pain on palpation • Pain at end range abduction, hand behind back • Scarf test • Pain provocation with horizontal adduction • NB restriction of movement may be due to posterior capsular stiffness esp. if scapular is held in retraction
Innervation • Suprascapular nerve • Nerve to Subscapularis • Axillary or Circumflex nerve • Lateral Pectoral Nerve • Autonomic Nervous System (LBHT)
Practical Session • Basic Assessment • Provocation Testing • Where to Start Rehab?
Indications for surgery • Pain • Loss of function and ROM • Quality of life • Failed conservative management • Age related considerations
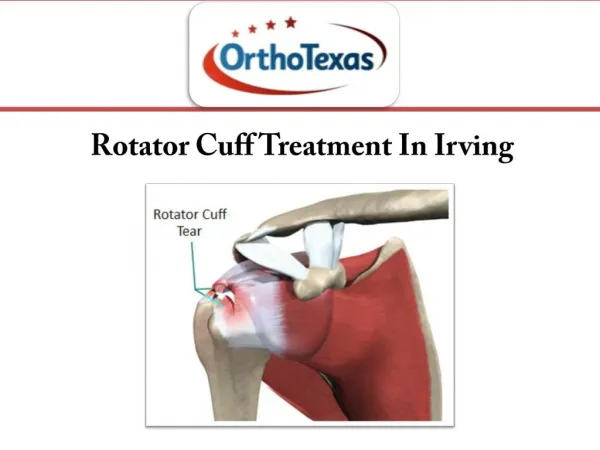
Pathology AVN Tumours Infection
Types of Shoulder Prosthesis • Fully constrained = For severe arthritis of the shoulder and destruction of the rotator cuff. Basically a salvage procedure. • Semi constrained = To prevent superior subluxation of the humeral prosthesis when the patient has joint arthritis and rotator cuff insufficiency. • Un Constrained =Joint arthritis with good rotator cuff function. • Surface replacement= one articular surface involved
Cemented Reduced pain reported Increased mobility Senior population Less physically demanding lifestyle Uncemented Avoid loosening of parts Scope for revision in younger person Active lifestyle Extended recovery period Cemented or Uncemented?
RNOH Philosophy • Bone Stock & Rotator Cuff • Good BS / good RC = unconstrained TSR • Good BS / poor RC = Constrained • Poor BS / good RC = CAD-CAM stem • Poor BS / poor RC = CAD-CAM glenoid/stem
Unconstrained Sulzar TSR – with glenoid liner (cemented) Glenoid screw and Biomet Humeral Component Modular (no glenoid liner) Cemented or uncemented
Constrained Reverse Delta-3
Constrained Reverse Fixed Fulcrum (Bayley-Walker)
Constrained CAD CAM
RNOH Rehabilitation guidelines Weak and smooth shoulder Stiff shoulder
Post operation immobilisation Abduction pillow polysling
Rehab GuidelinesAll of this will vary according to the individual Phase 1 – Initial Rehab Optimise tissue healing (time specified) Pain control “SMOOTH AND WEAK” Use of sling No ER>neutral/20 degrees A-A/Passive elevation<90 degrees No active use of UL or strengthening No HBB or cross body Education Milestones for next stage Achieved time specific goals For X-rays to show osseo-integration Allowed ROM achieved Reduced pain Adequate scapula control
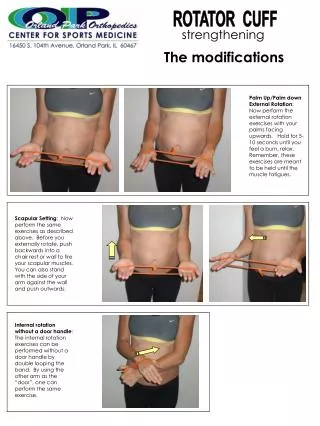
Early phase day 1 -6/52 exercise Active assisted GHJ FF 90 ISOMETRIC ER IN NEUTRAL Carer performing the exercise ISOMETRIC IR IN NEUTRAL
Early phase day 1 -6/52 exercise Start position with shoulder supported Carer performing the exercise End position of exercise Active assisted GHJ ER to neutral start…
Phase 2 – Early Recovery (approx 6 weeks – 4 months) Decrease sling use Start light activity at waist level Increase ROM Optimise normal movement patterns No exercises that increase pain No active anti-gravity work until RC rehabilitated Deltoid Programme for Constrained TSR Milestones for next stage No sling Minimal pain Passive ROM: elevation>90 and ER>30 RC stabilises within available ROM Functional Triangle
Phase 3 – Late Recovery (approx 5 months – 12 months) Increase strength and endurance to functional level required No exercises that increase pain No heavy lifting above shoulder level Milestones for Discharge Reduced pain from pre-op status Achieved functional goals Expected outcomes Unconstrained – Light to moderate use at waist, shoulder and above shoulder level Constrained – Light use at waist level and towards shoulder height if possible May take 12-24 months to achieve
Rehabilitation Guidelines • www.rnoh.nhs.uk • Follow link to CLINICAL SERVICES • Click on Physiotherapy • Click on SHOULDER AND ELBOW UNIT • Select Guideline for exercise information