Rotator Cuff Tear Algorithm
Rotator Cuff Tear Algorithm. Chelsea Kufahl Kayla Lingenfelter Amanda Livingston Brandon Smith. End point diagnosis: *Rotator Cuff Tear It could be this: *Tendonitis * Labral Tear *Impingement *Adhesive Capsulitis *Referred shoulder pain from other source. End point diagnosis.

Rotator Cuff Tear Algorithm
E N D
Presentation Transcript
Rotator Cuff Tear Algorithm Chelsea Kufahl Kayla Lingenfelter Amanda Livingston Brandon Smith
End point diagnosis: *Rotator Cuff Tear It could be this: *Tendonitis *Labral Tear *Impingement *Adhesive Capsulitis *Referred shoulder pain from other source End point diagnosis
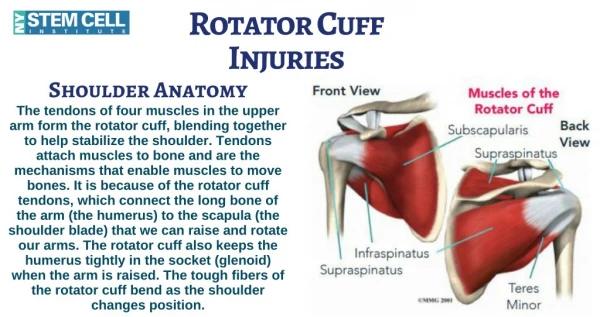
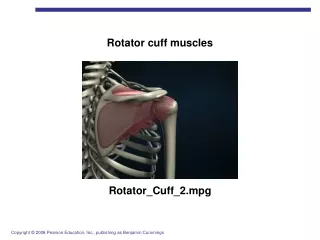
Supraspinatus Origin: Supraspinatus scapular fossa Insertion: Superior facet on greater tubercle of humerus Action: Initiates abduction at shoulder and externally rotates humerus Infraspinatus Origin: Infraspinatus scapular fossa Insertion: Middle facet on greater tubercle of humerus Action: Externally rotates the humerus Teres Minor Origin: Lateral border of scapula Insertion: Inferior facet on greater tubercle of humerus Action: Externally rotates humerus and weakly adducts the arm at shoulder Subscapularis Origin: Subscapular fossa and from lower 2/3 of lateral border of scapula Insertion: Lesser tubercle of humerus and anterior portion of shoulder joint capsule Action: Internally rotates and adducts the humerus at shoulder ***All four muscles draw the humerus toward the glenoid fossa , strengthening the shoulder joint Anatomy
Acute Tear: If you fall down on your outstretched arm or lift something too heavy with a jerking motion, you can tear your rotator cuff. This type of tear can occur with other shoulder injuries, such as a broken collarbone or dislocated shoulder. Degenerative Tear: Most tears are the result of a wearing down of the tendon that occurs slowly over time. This degeneration naturally occurs as we age. Several factors contribute to degenerative, or chronic, rotator cuff tears. • Repetitive stress. Repeating the same shoulder motions again and again especially overhead motions can stress your rotator cuff muscles and tendons. Overhead sports and many jobs and routine chores can cause overuse tears, as well. • Lack of blood supply. As we get older, the blood supply in our rotator cuff tendons lessens. Without a good blood supply, the body's natural ability to repair tendon damage is impaired. This can ultimately lead to a tendon tear. • Bone spurs. As we age, bone spurs (bone overgrowth) often develop on the underside of the acromion bone. When we lift our arms, the spurs rub on the rotator cuff tendon. This condition is called shoulder impingement, and over time will weaken the tendon and make it more likely to tear. Mechanism of Injury
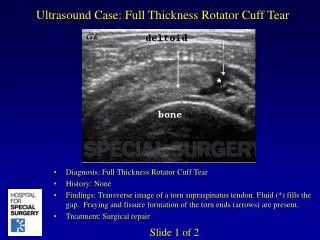
Partial Tear: This type of tear damages the soft tissue, but does not completely sever it. Full-Thickness Tear: This type of tear is also called a complete tear. It splits the soft tissue into two pieces. In many cases, tendons tear off where they attach to the head of the humerus. Rotator Cuff Tear
Age • As you get older, your risk of a rotator cuff injury increases. • Rotator cuff tears are most common in people > 40.
Poor Posture • Forward-Shoulder Posture • Can cause a muscle or tendon to become irritated and inflamed when you throw or perform overhead activities
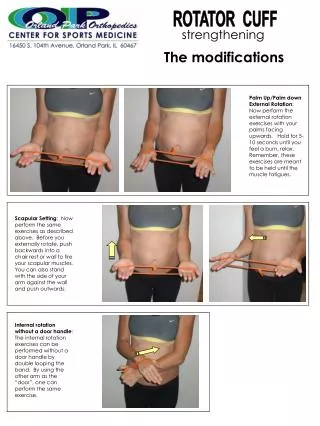
Weak Shoulder Muscles • Abductors and External Rotators • This risk factor can be decreased or eliminated with shoulder-strengthening exercises, especially for the less commonly strengthened muscles on the back of the shoulder and around the shoulder blades.
Repetitive Overhead Lifting • Athletes • tennis players • baseball pitchers • Occupation • painters • carpenters • others who do overhead work
Traumatic Injury • History of falls • History of any other shoulder injury
MOI • FOOSH with arm abducted or extended • Sudden jarring/sharp loading • Lifting from floor • O-linemen strike • Gradual onset d/t impingement and fraying • Location of Pain • Supraspinatus: outer aspect of shoulder to deltoid insertion, may radiate to elbow • Infraspinatus: posterior aspect of shoulder, may radiate down posterior arm • Subscapularis: local discomfort Signs and Symptoms
Description of Pain • Intermittent • At rest: superficial, local, anterior • After activity: deep ache, may radiate to elbow • AM/PM • Night pain • Can’t sleep on affected shoulder • Feeling of weakness • Can’t comb hair, reach into cabinet, lift light-mod weight items • Supraspinatus and ER specifically Signs and Symptoms
Observation • Atrophy of Muscle: Hollowed supraspinatus/infraspinatusfossa • Shoulder Hike: upper trap/deltoid compensation during movement • Limited AROM • Full PROM Signs and Symptoms
Empty Can Test • Drop Sign • Hand Behind Back – Lift Off Test • Hornblower Sign Primary Tests for Rotator Cuff Tear
Patient elevates shoulder to 90° of scaption with thumb pointed down. The clinician applies resistance. • Positive response is if there is weakness or pain in the supraspinatus region. • Test is indicative of supraspinatus tendonitis or a supraspinatus tear. Empty Can Test
The PT will passively move the patients arm to 90° of abduction with the elbow bent at 90°. • A positive sign is if the patient is unable to hold their arm in that position due to weakness and pain the rotator cuff area. • Test is indicative of infraspinatus tear. Drop Sign
The PT will put help the patient get into a position where they put the arm fully extended and internally rotated where they touch their lower back with the back of their hand. • A positive sign is if the patient is unable to lift the back of the hand off their back. • This is indicative of subscapularis weakness or tear. Hand Behind Back – Lift Off Test
The PT will put patient’s arm in 90° of abduction in scapular plan. The elbow is flexed at 90°. The patient will try to ER forearm against the resistance of the PT. • A positive sign is if the patient cannot externally rotate their arm, and they assume a position of a positive hornblower sign. • This test is indicative of teres minor tear. Hornblower Sign
Subacromial Impingement Tests • Hawkins-Kennedy Impingement Test • Supraspinatus tendon impingement • Can be positive if have a rotator cuff tear. • Neer’s Test • Supraspinatus tendon impingement • Labral Tear Tests • Crank Test • SLAP lesions • Speed’s Test • Superior labral tear / Bicipital tendonitis • O Brien’s Test • Labral tear Other Tests to Perform
Shoulder Stability Tests • Sulcus Sign • Multidirectional instability/inferior stability • Load and Shift Test • Anterior and posterior instability of glenohumeral joint • Apprehension Test • Anterior instability • Relocation Test • Anterior instability Other Tests to Perform
This algorithm can assist physical therapists by giving them a set of steps to follow if their patient is displaying the signs and symptoms associated with a rotator cuff tear. The physical therapist can then follow the steps in the algorithm to come to a diagnosis for their patient and treat them accordingly. TAKE HOME MESSAGE
Burbank, K. M., J. H. Stevenson, G. R. Czarnecki, and J. Dorfman. "Chronic Shoulder Pain: Part I. Evaluation and Diagnosis." American Family Physician 77.4 (2008): 453-60. Print. • Loudon, J, Swift, M. & Bell, S. (2008) The Clinical Orthopedic Assessment Guide (2nd ed). Champaign, IL: Human Kinetics. • Murrell, G. A., & Walton, J. R. (2001). Diagnosis of rotator cuff tears. Lancet, 357(9258), 769–70. doi:10.1016/S0140-6736(00)04161-1 • OrthoInfo. (2011). Rotator Cuff Tears. Retrieved from http://orthoinfo.aaos.org/topic.cfm?topic=a00064. • Jain, N. B., Wilcox, R. B., Katz, J. N., & Higgins, L. D. (2013). Clinical examination of the rotator cuff. PM & R : the journal of injury, function, and rehabilitation, 5(1), 45–56. doi:10.1016/j.pmrj.2012.08.019 • Yamamoto, A. (n.d.). Prevalence and risk factors of a rotator cuff tear in the general population. (2010). Journal of Shoulder and Elbow Surgery, 19(1), 116-120. Retrieved from http://www.sciencedirect.com/science/article/pii/S1058274609002043 References