Download

1 / 106
1.09k likes | 1.46k Vues
Disorders of Absorption. Introduction. Broad spectrum of conditions with multiple etiologies and varied clinical manifestations.

E N D
Introduction • Broad spectrum of conditions with multiple etiologies and varied clinical manifestations. • Almost all of these clinical problems are associated with diminished intestinal absorption of one or more dietary nutrients and are often referred to as the malabsorption syndrome
steatorrhea Most, but not all, malabsorption syndromes are associated with steatorrhea, an increase in stool fat excretion of >6% of dietary fat intake
Malabsorption disorders are not associated with steatorrhea • primary lactase deficiency, a congenital absence of the small intestinal brush border disaccharidase enzyme lactase, is associated with lactose "malabsorption, • pernicious anemia is associated with a marked decrease in intestinal absorption of cobalamin (vitamin B12) due to an absence of gastric parietal cell intrinsic factor required for cobalamin absorption.
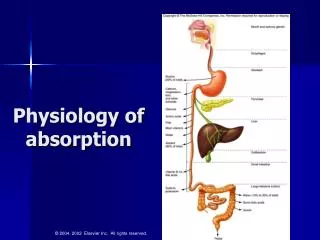
Nutrient Digestion and Absorption • The lengths of the small intestine and colon are ~300 cm and ~80 cm, respectively. • The effective functional surface area is approximately 600-fold greater than that of a hollow tube as a result of the presence of folds, villi (in the small intestine), and microvilli
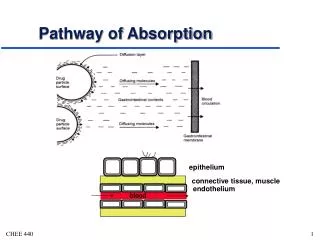
Intestinal epithelia several other functions: • Barrier and immune defense. The intestine is exposed to a large number of potential antigens and enteric and invasive microorganisms, and it is extremely effective preventing the entry of almost all these agents. • The intestinal mucosa also synthesizes and secretes secretory IgA.
Intestinal epithelia several other functions • Fluid and electrolyte absorption and secretion. The intestine absorbs ~7–8 L of fluid daily, comprising dietary fluid intake (1–2 L/d) and salivary, gastric, pancreatic, biliary, and intestinal fluid (6–7 L/d). • Several stimuli, especially bacteria and bacterial enterotoxins, induce fluid and electrolyte secretion that may lead to diarrhea
Intestinal epithelia several other functions • Synthesis and secretion of several proteins. The intestinal mucosa is a major site for the production of proteins, including apolipoproteins • Production of several bioactive amines and peptides. The intestine is one of the largest endocrine organs in the body and produces several amines and peptides that serve as paracrine and hormonal mediators of intestinal function
The small and large intestines are distinct anatomically (villi are present in the small intestine but are absent in the colon) and functionally (nutrient digestion and absorption take place in the small intestine but not in the colon).
No precise anatomic characteristics separate duodenum, jejunum, and ileum, although certain nutrients are absorbed exclusively in specific areas of the small intestine
lipid • Steatorrhea is caused by one or more defects in the digestion and absorption of dietary fat. • Average intake of dietary fat in the United States is approximately 120–150 g/d, and fat absorption is linear to dietary fat intake. • The total load of fat presented to the small intestine is considerably greater, as substantial amounts of lipid are secreted in bile each day
Defects in Lipid Digestion and Absorption in Steatorrhea
Lipolysis, micelle formation, and lipid uptake are all normal in patients with abetalipoproteinemia, but the reesterified triglyceride cannot exit from the epithelial cell because of the failure to produce chylomicrons. Small-intestinal biopsies of these rare patients in the postprandial state reveal lipid-laden small-intestinal epithelial cells that become perfectly normal in appearance following a 72–96 h fast
Comparison of Different Types of Fatty Acids
Medium cahin triglyceride • Medium-chain triglycerides (MCTs), composed of fatty acids with carbon chain lengths of 8–10, are present in large amounts in coconut oil and are used as a nutritional supplement. • MCTs can be digested and absorbed by a different pathway from LCTs and at one time held promise as an important treatment of steatorrhea of almost all etiologies. • Unfortunately, their therapeutic effects have been less than expected because their use is often not associated with an increase in body weight for reasons that are not completely understood.
Medium cahin triglyceride • MCTs are absorbed more efficiently than LCTs for the following reasons: • (1) the rate of MCT absorption is greater than that of long-chain fatty acids; • (2) following absorption are not reesterified; • (3) following absorption, MCTs are hydrolyzed to medium-chain fatty acids; • (4) MCTs do not require chylomicron formation for their exit from the intestinal epithelial cells; • (5) their route of exit is via the portal vein and not via lymphatics.
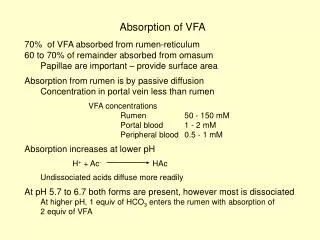
Short chain fatty acid • SCFAs are not dietary lipids but are synthesized by colonic bacterial enzymes from nonabsorbed carbohydrate and are the anions in highest concentration in stool (between 80 and 130 mM). • The SCFAs present in stool are primarily acetate, propionate, and butyrate, whose carbon chain lengths are 2, 3, and 4, respectively. Butyrate is the primary nutrient for colonic epithelial cells, and its deficiency may be associated with one or more colitides.
Short chain fatty acid • SCFAs conserve calories and carbohydrate, because carbohydrates not completely absorbed in the small intestine will not be absorbed in the large intestine due to the absence of both disaccharidases and SGLT1, the transport protein that mediates monosaccharide absorption. In contrast, SCFAs are rapidly absorbed and stimulate colonic Na-Cl and fluid absorption.
Most non–Clostridium difficile antibiotic-associated diarrhea is due to antibiotic suppression of colonic microflora, with a resulting decrease in SCFA production. • As C. difficile accounts for about 10–15% of all antibiotic-associated diarrhea, a relative decrease in colonic production of SCFAs is likely the cause of most antibiotic-associated diarrhea.
Carbohydrates • Carbohydrates in the diet are present in the form of starch, disaccharides (sucrose and lactose), and glucose. • Carbohydrates are absorbed only in the small intestine and only in the form of monosaccharides.
Carbohydrates • Before their absorption, starch and disaccharides must first be digested by pancreatic amylase and intestinal brush border disaccharidases to monosaccharides. • Monosaccharide absorption occurs by a Na-dependent process mediated by the brush border transport protein SGLT1.
Lactose malabsorption • Lactose malabsorption is the only clinically important disorder of carbohydrate absorption. • Lactose, the disaccharide present in milk, requires digestion by brush border lactase to its two constituent monosaccharides, glucose and galactose. • In primary lactase deficiency, a genetically determined decrease or absence of lactase is noted, while all other aspects of both intestinal absorption and brush border enzymes are normal
Lactose malabsorption • secondary lactase deficiency occurs in association with small-intestinal mucosal disease with abnormalities in both structure and function of other brush border enzymes and transport processes. Secondary lactase deficiency is often seen in celiac sprue
lactose malabsorption • Some individuals with lactose malabsorption develop symptoms such as diarrhea, abdominal pain, cramps, and/or flatus. • Most individuals with primary lactase deficiency do not have symptoms. • Since lactose intolerance may be associated with symptoms suggestive of irritable bowel syndrome, persistence of such symptoms in an individual with lactose intolerance while on a strict lactose-free diet would suggest that the individual's symptoms were related to irritable bowel syndrome.
Proteins • Protein is present in food almost exclusively as polypeptides and requires extensive hydrolysis to di- and tripeptides and amino acids before absorption. • Proteolysis occurs in both the stomach and small intestine; it is mediated by pepsin secreted as pepsinogen by gastric chief cells and trypsinogen and other peptidases from pancreatic acinar cells. • Proteins are absorbed by separate transport systems for di- and tripeptides and for different types of amino acids, e.g., neutral and dibasic
Disease with malabsorption must be suspected in individuals with less severe symptoms and signs and with subtle evidence of the altered absorption of only a single nutrient rather than obvious evidence of the malabsorption of multiple nutrients.
Dietary nutrient absorption may be segmental or diffuse along the small intestine and is site-specific.Calcium, iron, and folic acid are exclusively absorbed by active transport processes in the proximal small intestine, especially the duodenum
Active transport mechanisms for both cobalamin and bile acids are present only in the ileum.Glucose, amino acids, and lipids, are absorbed throughout the small intestine, though their rate of absorption is greater in the proximal than in the distal segments
Differential Results of Schilling Test in Several Diseases Associated with Cobalamin (CBL) Malabsorption
Urinary D-Xylose Test • The urinary D-xylose test for carbohydrate absorption provides an assessment of proximal small-intestinal mucosal function. D-Xylose, a pentose, is absorbed almost exclusively in the proximal small intestine. The D-xylose test is usually performed by giving 25 g D-xylose and collecting urine for 5 h. • An abnormal test (<4.5 g excretion) primarily reflects the presence of duodenal/jejunal mucosal disease.
Urinary D-Xylose Test • The D-xylose test can also be abnormal in patients with blind loop syndrome (as a consequence primarily of abnormal intestinal mucosa) and, as a false-positive study, in patients with large collections of fluid in a third space (i.e., ascites, pleural fluid). The ease of obtaining a mucosal biopsy of the small intestine by endoscopy and the false-negative rate of the D-xylose test have led to its diminished use. • When small-intestinal mucosal disease is suspected, a small-intestinal mucosal biopsy should be performed
Radiologic Examination • A normal barium contrast study does not exclude the possibility of small-intestinal disease. • small-bowel series remains a useful examination to look for anatomical abnormalities, such as strictures and fistulas (as in Crohn's disease) or blind loop syndrome (e.g., multiple jejunal diverticula), and to define the extent of a previous surgical resection. • Noninvasive capsule endoscopy and double-barrel enteroscopy are useful aids in the diagnostic assessment of small intestinal pathology.
Biopsy of Small-Intestinal Mucosa • A small-intestinal mucosal biopsy is essential in the evaluation of a patient with documented steatorrhea or chronic diarrhea (lasting >3 weeks). • The primary indications for a small-intestinal biopsy are (1) evaluation of a patient either with documented or suspected steatorrhea or with chronic diarrhea, and (2) diffuse or focal abnormalities of the small intestine defined on a small-intestinal series
MALABSORBTION CELIAC DISEASE
EPIDEMIOLOGY • The picture changed in the 1970s with rising awareness of the often oligosymptomatic form of celiac disease and the advent of sensitive and specific serologic assays for IgA antibodies to gliadin and endomysium.
EPIDEMIOLOGY • Epidemiological studies using these tests with biopsy verification established higher prevalences of 1:300 to 1:500 in most countries. • Studies in 2000 American blood donors, for example, suggest a prevalence of 1:250 based upon endomysial antibody testing
EPIDEMIOLOGY • In a report from Denmark, screening assays increased the prevalence from 1:10,000 to 1:300 • These findings indicate that the number of so-called silent celiacs (a misnomer, since most of these patients suffer from nonspecific symptoms) is much higher than the number of patients with classic celiac disease.
Etiology • The etiology of celiac sprue is not known. • One environmental factor is the clear association of the disease with gliadin, a component of gluten that is present in wheat, barley, and rye. • In addition to the role of gluten restriction in treatment, the instillation of gluten into both normal-appearing rectum and distal ileum of patients with celiac sprue results in morphologic changes within hours.
Etiology • An immunologic component to etiology is suspected. Serum antibodies—IgA antigliadin, IgA antiendomysial, and IgA anti-tTG antibodies—are present, but it is not known whether such antibodies are primary or secondary to the tissue damage
Genetic factors • Intrafamilial occurrence and the remarkably close association with the HLA-DQ2 and/or DQ8 gene locus • HLA typing for DQ2 and DQ8 may be useful in individuals with equivocal small bowel histologic findings since celiac disease is unlikely if neither is present
Serum autoantibodies • IgA endomysial antibody (IgA EMA) • IgA tissue transglutaminase antibody (IgA tTG) • IgA antigliadin antibody (IgA AGA) • IgG antigliadin antibody (IgG AGA)