Introduction Anemia classification based on the mechanism
760 likes | 1.08k Vues
MACROCYTIC ANEMIAS Ahmad Sh. Silmi Staff Specialist in Haematology Medical Laboratory Sciences Dept, IUG 2012. Introduction Anemia classification based on the mechanism. Kinetic Classification (based on retic count) Decreased production Morpholgical classification (based on MCV)

Introduction Anemia classification based on the mechanism
E N D
Presentation Transcript
MACROCYTIC ANEMIASAhmad Sh. SilmiStaff Specialist in HaematologyMedical Laboratory Sciences Dept, IUG 2012
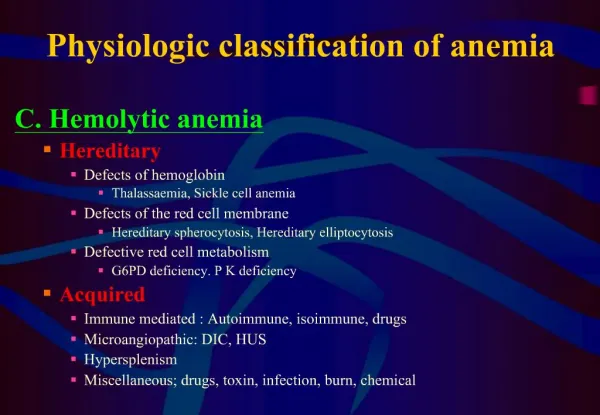
IntroductionAnemia classification based on the mechanism • Kinetic Classification(based on retic count) • Decreased production • Morpholgical classification (based on MCV) • Microcytic • Normocytic • Macrocytic • Increased destruction • Immunological classification(based on Coomb’s test) • Immune-mediated • Non-immune mediated
The Medical Student’s Approach to Anemia • Check the reticulocyte count to determine if the anemia is from decreased production (“hypoproliferative”, “reticulocytopenic”) or increased destruction (“hemolytic”)/acute blood loss (“reticulocytosis”) 2. If decreased production, narrow down the causes in terms of the MCV- • If the MCV is low, then do iron studies then Hb electropheresis • If the MCV is normal, check the serum creatinine and TSH, if they are WNL then consider bone marrow exam • If the MCV is high check a folate and vitamin B12 level 3. If the reticulocyte count is increased- • Check a direct Coomb’s test 4. Look at the peripheral blood smear to confirm/support the diagnosis
Big Issue‼ • MCV=mean corpuscular volume
Anemia Algorithm • Patient with anemia and decreased reticulocyte count- What is the MCV ?? Normocytic • Macrocytic: • Vitamin-related • B12,Folate • Non-vitamin: • MDS • EtOH/Liver Disease • Hypothyroidism Microcytic • Diseases in Bone Marrow • MDS • Solid Tumor • Myeloma • Aplastic anemia Fe def. Systemic Diseases Thal Renal vs. Liver vs. Endocrine vs. Anemia of Inflammation Other: sideroblastic anemia
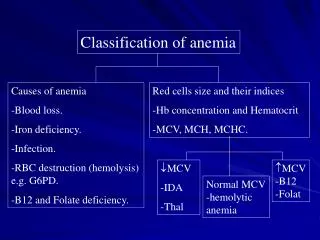
Anemia : MCV >100 Macrocytic Defective DNA synthesis Megaloblastic anemia B12 deficiency Folate deficiency Myelodysplastic Syndromes Young RBCs-reticulocytosis Hemolytic anemia Hypoplastic anemias Aplastic anemia 80-100 Normocytic Decreased production Aplastic anemia Increased destruction Acute blood loss Hemolytic anemias Acquired Autoimmune HA Infectious disease Inherited Membrane defects Hereditary spherocytosis Hereditary elliptocytosis Enzyme defect/deficiency Glucose 6 phosphate dehydrogenase Pyruvate kinase Unstable hemoglobin <80 Microcytic Defective hemoglobin synthesis Iron deficiency (Fe2+) Thalassemia (globin chain) Sideroblastic anemia (heme) Low Reticulocyte index High
Requirements for Red Blood Cell Production • Erythropoeitin • Proteins, required for globin synthesis • Iron • Vitamin B12 and folic acid • Vitamin B6 • Vitamin C • Thyroid hormones, estrogens and androgens
Definitions • Macrocytic • MCV > 100 • MCH is increased due to increased cell size • MCHC is normal as concentration of hemoglobin is normal • Macrocytosis is found in 2.5-4% of adults having a routine CBC • Sub classification • Megaloblastic • Non-megaloblastic
Megaloblastic More severe macrocytosis with oval erythrocytes Usually MCV is >110 Defects in DNA syntheses leading to delayed nuclear development in the face of normal cytoplasmic development Marrow shows nuclear cytoplasmic asynchrony Erythroid lineage Myeloid lineage Reticulocyte index is not increased Non-Megaloblastic Less severe macrocytosis with round erythrocytes Usually MCV is <110 Pathophysiology unknown Increase in membrane lipids Immature cells (reticulocytes) are increased Macrocytic anemias
Megaloblastic B 12 deficiency Folate deficiency Drugs Megaloblastoid morphologic changes can be seen in Myelodysplastic syndromes Congenital dyserythropoietic anemias Non-Megaloblastic Alcoholism Liver disease Hypothyroidism Aplastic anemia Hemolysis, acute bleed Increased reticulocytes and immature erythrocytes Artifact RBC clumping cold agglutinin disease Hyperglycemia RBC swelling Macrocytic anemias * * *
MEGALOBLASTIC ANEMIA • These are a group of disorders in which the cause the anemia is due to deficiency of vitamin B12 and folic acid • The macrocytes in this condition is usually “oval” - hence they are also called as MACRO OVALOCYTES
NON MEGALOBLASTIC MACROCYTIC ANEMIAS • These are disorders in which the macrocytosis is not due to vitamin B12 or folic acid deficiency • Here the macrocytes are “ROUND” • The conditions in which such round macrocytes are seen are • Reticulocytosis • Hypothyroidism / myxedema • Myelodysplastic syndrome • Scurvy (Vit-C dif) • Sideroblastic anemia • Liver disorders
MEGALOBLASTIC ANEMIA • Vitamin B12 and folic acid are important nutrients required in the process of nuclear maturation • They are required during erythropoiesis (during DNA synthesis) • These anemias may be caused because of a nutritional deficiency or impaired absorption mainly.
MEGALOBLASTIC ANEMIA • Impaired DNA synthesis leading to defective cell maturation and cell division • Nuclear maturation delays from the cytoplasmic maturation – NUCLEAR CYTOPLASMIC ASYNCHRONY • Abnormally large erythroid precursors and red cells
Folic Acid: • It a vitamin which is yellow in colour, water soluble, necessary for the production of the RBC, WBC and platelets. • It is not synthesized in the body. • It is found in large number of green fresh vegetables, fruits. • Daily requirement: The human body needs about 100-150 µg daily. Absorption: It is absorbed in the Duodenum and Jejunum. • Transportation: Weakly bound to albumin.
METABOLIC FUNCTION • Purine synthesis • Conversion of homocysteine to methionine ( which also requires B12 )
FOLIC ACID DEFICIENCY • INCREASED DEMAND • DECREASED INTAKE • DECREASED ABSORPTION • METABOLIC INHIBITION
INCREASED DEMAND • Pregnancy • Lactation • Infancy • Puberty and growth period • Patients with chronic hemolytic anemias • Disseminated cancer
DECREASED INTAKE • Elderly • Lower socio economic status • Chronic alcoholics
DECREASED ABSORPTION • Acidic food substances in foods like legumes, beans • Drugs like phenytoin, oral contraceptives • Celiac disease which affect the gut absorption • Heat sensitive – more loss during cooking
Vitamin B12: • This vitamin is synthesized in nature by micro-organism in the intestine of man and animals, but we can not obtain it from the bacteria in our bodies, because it is synthesizing in the large colon after the site of absorption and it is wasted in the faeces in about 5µg/day. So we obtain it from animal food such as liver, kidney, meat and dairy products as milk and cheese.
VITAMIN B12 • Abundant in animal foods • Microorganisms are the ultimate origin of cobalamin • It is stored in liver for many years • It is efficiently reabsorbed from bile • It is resistant to cooking and boiling
Diary requirements: The human body needs about 1-2 µg daily. • Absorption: B12 is combined with glycoprotein called the intrinsic factor (IF), which is synthesized in the gastric cells. The absorption occurs in the distal ileum. • Transportation: Transport by a protein synthesized in the liver called Transcobalamine II, which carry vitamin B12 to liver, nerves and bone marrow.
VITAMIN B12 DEFICIENCY • INCREASED REQUIREMENT • DECREASED INTAKE • IMPAIRED ABSORPTION
INCREASED DEMAND • Pregnancy • Lactation • Puberty • Growth period • Hyperthyroidism • Disseminated cancer
DECREASED INTAKE • Inadequate intake • Vegetarian diet
IMPAIRED ABSORPTION • INTRINSIC FACTOR DEFICIENCY due to chronic gastritis or antibodies against stomach cells. - PERNICIOUS ANEMIA - GASTRECTOMY • Malabsorption states • Diffuse intestinal diseases. Eg., lymphoma, systemic sclerosis • Competitive parasitic uptake – fish tapeworm • Bacterial overgrowth
Pathophysiology Folates are compounds derived from folic acid that are involved in numerous metabolic reactions Generally folates act as donor of single carbon groups dUMP=deoxyuridylate monophosphate DTMP=deoxythymidylate monophosphate One such reaction is thymidylate synthesis Defective thymidylate synthesis leads to defective DNA synthesis Megaloblastic anemia
B12 and folate • B12 is a known cofactor in 2 enzymatic reactions • (1) B12 is a cofactor of methionine synthase which is required to regenerate folate within the cell
Other sequelae of B12 deficiency • (2) Conversion ofmethylmalonyl CoA and finally to succinyl-CoA • Co factor for methylmalonyl CoA • Failure of this pathway leads to abnormalities in neuronal membrane synthesis. • Also, methionine is a precursor for S-adenosylmethionine-a metabolite critical for normal function of the nervous system. • Neurologic defects seen with B12 deficiency • Peripheral neuropathy • Disturbances of vibratory sense and proprioception • Dorsal and lateral column demyelination • Spastic ataxia • Brain • Dementia, psychosis, somnolence • Although anemia may respond to folate therapy, neurologic findings will not • Neurologic findings may be permanent if not treated early 1 Up-to-Date
Folate deficiency • Dietary sources • Present in animal and vegetable products • Asparagus, broccoli, spinach, lettuce, lima beans (>1mg/100g dry weight) • Liver, yeast, mushrooms, oranges • Cooking depletes food of folate • Metabolism • Absorbed most actively in the jejunum and upper ileum • Body stores are 5-10 mg (liver) • Minimal daily intake is 50 micrograms • Higher for pregnancy and lactation • Folate deficiency can lead to birth defects (neural tube defects) • If intake is reduced to 5 micrograms/day, megaloblastic anemia will develop in ~4 months
Folate deficiency • Causes of folate deficiency • Decreased intake (most common) • Dietary deficiency • Infants on a Goat’s milk diet • Small intestinal disease • Tropical sprue • Celiac sprue (gluten sensitive enteropathy) • Increased requirement • Pregnancy • Alcoholism • Hemolytic anemia • Leukemia
B12 deficiency • Dietary sources • Animal products (meat and dairy) • Metabolism • Ingested B12 is protein bound • Trypsin and acid in stomach release B12 • B12 binds R-binding protein which carries it to the jejunum • Also in the stomach (fundus and body) intrinsic factor is secreted. • In the jejunum, pepsin releases B12 from R-binding protein • B12 binds intrinsic factor and is carried to the ileum • B12 is absorbed in the ileum • Body stores 2-5mg (mostly in the liver) • Need 3-5 micrograms per day for maintenance of stores • Increased need in pregnancy, lactation, growth • Depletion takes longer that folate • It takes years to develop megaloblastic anemia due to B12 deficiency
B12 deficiency • Decreased intake • Veganism • Impaired absorption • Gastric • Poor stomach acidity • Gastrectomy • Pernicious anemia • Decreased secretion of intrinsic factor due to gastric atrophy • Chronic pancreatitis • Decreased digestive enzyme secretion • Intestinal disease • Ileal resection • Ileal disease • Chron’s disease • Celiac sprue • Fish tapeworm • Diphyllobothrium latum • Blind loop • Intestinal bacterial overgrowth
Diagnosis Homocystine • Clinical findings • Morphology-peripheral blood and marrow • Megaloblastoid morphologic changes • Folate deficiency • Folate, serum level • Reflects recent levels of ingestion • Falsely increased with hemolysis • RBC Folate • Reflects stores (2-3 months) • Will be decreased in B12 deficiency • B12 deficiency • Folate levels are decreased in B12 deficiency, should check both in tandem • B12, serum level • Serum methylmalonic acid and homocystine levels may be more sensitive • B12 deficiency, both are elevated • sensitivity 94%, specificity 99% • Folate deficiency, only homocystine levels are elevated • sensitivity 94%, specificity 99% • May miss 10-26% of patients with serum B12 levels alone • Schillings test • Helps to identify the source of B12 deficiency MMA
Sequence of changes in megaloblastic anemia • Vitamin levels decrease • Neutrophil hypersegmentation • Oval macrocytosis in the peripheral blood • Megaloblastic changes in the marrow • Anemia
MEGALOPLASTIC ANAEMIA. • Affect all marrow elements. • Neurologic symptoms (dorsal columns) • Ineffective erythropoiesis:High indirect bilirubinVery high LDH
Ineffective hematopoiesis • Because of the faulty megaloblastic maturation seen in the marrow, cells die during cell division • Hypercellular marrow due to erythroid hyperplasia with increased red blood cell precursors in the marrow but a macrocytic anemia in the periphery • Release of cell constituents • Increased bilirubin • Increased LDH
CLINICAL FEATURES • Patients develop all general symptoms and signs of the anaemia. • Knuckle pigmentation • Angular stomatitis • Atrophic glossitis- “beefy” tongue • Neurological disorders: sever deficiency of the folic acid causes neuropathies diseases. • Deficiency during pregnancy causes neural tube defect.
Schillings test Allows one to determine the level at which B12 deficiency is occurring Dietary deficiency Malabsorption Absence of intrinsic factor
Screening hematology laboratory tests for megaloblastic anemia • CBC • Macrocytic anemia • MCV is usually >110 fL and often >120 fL • Pancytopenia is seen in some cases • Peripheral blood morphology • Oval macrocytes • Nucleated RBCs, Howell Jolly bodies, basophilic stippling, Cabot rings • Neutrophil nuclear hypersegmentation • five 5 lobed neutrophils per 100 WBC • One six lobed neutrophil
Peripheral blood Macro-ovalocytes Neutrophil nuclear hypersegmentation Very sensitive and specific Megaloblastic anemia: Morphology--Blood Megaloblastoid Normal
Cabot ring - Ring shaped, thin - May be figure of 8 shaped - Microtubule, remnants of of themitotic spindle - Rarely seen Howell Jolly body - Round, dark, refractile RBC inclusion - Nuclear remnant - Most commonly seen in hyposplenism Basophilic stippling - Multiple small blue dots dispersed regularly throughout the RBC - RNA complexes
PERIPHERAL BLOOD FINDINGS • Hemoglobin – decreased • Hematocrit – decreased • RBC count – decreased/normal • MCV - >100fl ( normal 82-98fl) • MCH –increased • MCHC – NORMAL • Reticulocytopenia. • Total WBC count – normal / low • Platelet count – normal/ low • Pancytopenia, especially if anaemia is sever.
PERIPHERAL SMEAR • RBC: • Poikilocytosis - tear drops and schistocytes • Anisocytosis - oval macrocytes -Macro ovalocytes (macrocytic normochromic) -well hemogloibised, thicker than normal -inclusions like HOWELL JOLLY BODIES, basophilic stippling, Cabot rings
PERIPHERAL SMEAR • WBC: Normal count or reduced count Hypersegmented neutrophils (>5 lobes) MACRO POLYMORPHO NUCLEAR CELLS (Macropolys) • PLATELETS: Normal or decreased