Classification of anemia
300 likes | 2.87k Vues
Classification of anemia. Causes of anemia -Blood loss. -Iron deficiency. -Infection. -RBC destruction (hemolysis) e.g. G6PD. -B12 and Folate deficiency. Red cells size and their indices -Hb concentration and Hematocrit -MCV, MCH, MCHC. MCV -IDA -Thal. MCV -B12 -Folat .

Classification of anemia
E N D
Presentation Transcript
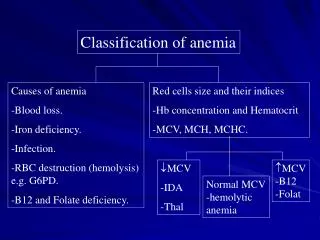
Classification of anemia Causes of anemia -Blood loss. -Iron deficiency. -Infection. -RBC destruction (hemolysis) e.g. G6PD. -B12 and Folate deficiency. Red cells size and their indices -Hb concentration and Hematocrit -MCV, MCH, MCHC. • MCV -IDA -Thal • MCV -B12 -Folat Normal MCV -hemolytic anemia
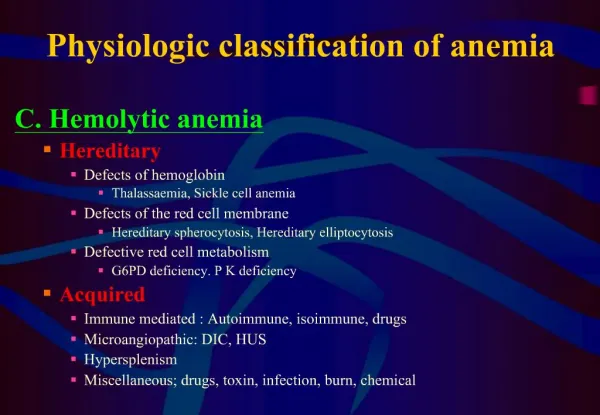
Iron deficiency anemia Normal iron metabolism: -The primary function is oxygen transport. -Iron is absorbed by duodenum and jejunim -Average total body iron content 3500-4000 mg. -Approximately 2/3 found in hemoglobin, -Iron is also stored in RE cells (BM, Spleen and liver) as hemosiderin and ferratin. -Also iron found in myglobin and myeloperoxidase and in certain electron transfer. -Iron is more stable in ferric state (Fe+++) than in ferrous state (Fe++).
Iron + Hem Iron Metabolism
Daily Fe++ turnover continuous process RBC 2500 mg 20 mg Fe Returned to immature RBC in BM R.E. 20 mg Released daily Via RE system 90% extra vascular 5-10% intra vascular Iron Absorption 1-2 mg only Plasma Fe Transferrin carriers 4 mg Loss (from GI tract) 1-2 mg daily Body stores 1000 mg (M) 300-500 mg (F) Myglobin 300 mg
Dietary iron: Iron is present in food as ferric hydroxides (ferric-protein complexes and hem-protein complexes). -meat, liver -vegetables, eggs. -The average diet contains 10-15mg and only 5-10% is normally absorbed. Iron requirements: It varies depending on sex and age: Male/female 0.5-1 mg/day Pregnant female 1-2 mg/day Children 0.5 mg/day
Clinical features: • When ID is developing, the RE stores (hemosiderin and ferritin) become completely depleted before anemia occurs. • At an early stage, no clinical abnormalities. • Later, patient may develops general symptoms and signs of anemia. • In severe case of IDA ridged or spoon nails.
Causes: • Chronic blood loss • Fetomaternal Hemorrhage, inherited bleeding disorders menstrual peroid. • Maternal iron deficiency (neonate). • Growth spurts (infants and children). • Gastrointestinal, • peptic ulcer, aspirin ingestion, carcinoma, hookworm, colitis, piles etc. • Pregnancy • Rarely hematouria, • self-inflicted blood loss, hemoglobinuria. • Insufficient daily iron intake (poor diet). • Malabsorption.
Laboratory findings: • Red cell indices: • Low Hb conc. • MCV, MCH, MCHC* • Blood film: • Hypochromic microcytic Picture. • Occasional Target cells. • Pencil shaped poikilocytes. • Normal reticulocyte count. • Bone marrow iron: • Normal to hypercellular. • RBC precursors are increased in number. • Iron stain negative. • Chemical testing on serum: • Serum iron Decreased • Transferrin/TIBC Normal to High • Serum ferritin Decreased (Very low)
Hypochromic Microcytic picture (IDA) -ve BM Iron Stain +ve