Metabolite Kinetics Theoretical Approach
230 likes | 458 Vues
Metabolite Kinetics Theoretical Approach. PHM324Y Guest Lecturer Dr. Jasmina Novakovic Apotex Inc, R&D. To be consistent with other slide packs, in this slide pack kfm should be km. Where kfm appears a note identifying the change has been added. Learning Objectives. Drug fate

Metabolite Kinetics Theoretical Approach
E N D
Presentation Transcript
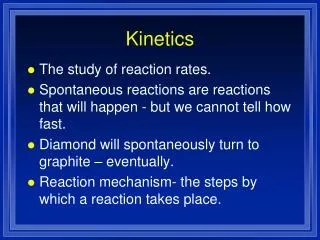
Metabolite KineticsTheoretical Approach PHM324Y Guest Lecturer Dr. Jasmina Novakovic Apotex Inc, R&D To be consistent with other slide packs, in this slide pack kfm should be km. Where kfm appears a note identifying the change has been added. November 2007
Learning Objectives • Drug fate • Renal and hepatic elimination • Drug-metabolite relationships • Fundamentals of metabolite kinetics • Metabolite concentration versus time profile • Estimation of relevant rate constants November 2007
Drug Fate • Elimination = clearance • How? • Unchanged or metabolized. • Where? • Excreta. Urine, bile, feces, perspiration… • Clearance renal, mainly unchanged drug • Clearance hepatic = metabolic clearance • Other clearances (e.g. bile) • Liver - the main site of biotransformation. More that one metabolite can be formed: CLh = CLm1 + CLm2+… • CLtotal = CLh + CLr + CLother November 2007
Drug-Metabolite RelationshipsImportant Facts • Drug = precursor • Metabolite = successor • As long as precursor is in the body, the successor will be there • Half-life of a metabolite formed from the drug can not be shorter than parent drug’s half-life • Conc-time profile of a metabolite: One exponent more than conc-time profile of the parent drug • Metabolite is a chemically distinct entity and has its own volume of distribution and clearance November 2007
Relationship Between Drug and Metabolite(A) i.v. Doses Given on Separate Occasions November 2007
What Can We Learn from i.v. Data? • The only way to determine Vd of metabolite. • Metabolite, when given individually, can have longer or shorter T1/2 than drug. What will be if the metabolite is formed in the body? November 2007
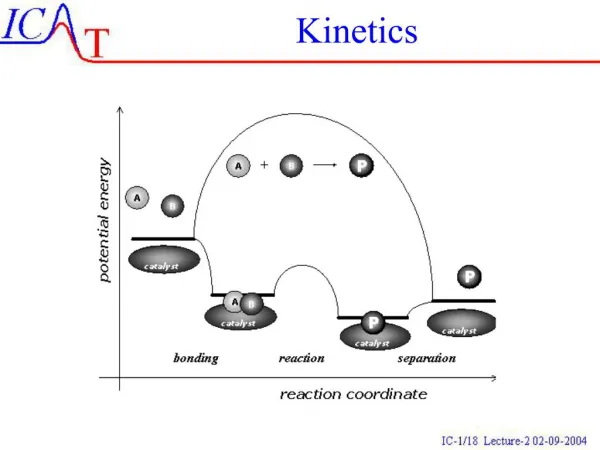
Relationship Between Drug and Metabolite(B) Drug was given i.v., the metabolite is formed Analogy between oral absorption and metabolism Drug in the body ka Drug at absorption site K Absorption Elimination of Drug km Metabolite in the body kme Drug in the body kfm Elimination of Metabolite Metabolism As long as the drug is in the body, the metabolite will be formed. What would be Plasma Conc versus Time profile of metabolite? November 2007
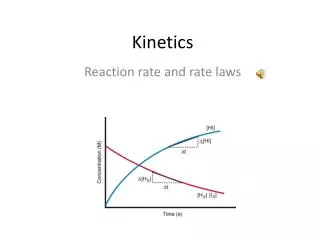
Drug: i.v. bolus, mono-exponential conc vs time profile Metabolite: Polar, no further metabolites Urine IV Dose (Ao) ke A Drug Vd Bile kb kme Metabolite Vm kmf dA/dt= -K A K = ke + kmf+ kb At = Aoe-Kt /Vd Ct = Co e-Kt dM/dt = kmf A – kme M Mt = kmf Ao[ e-Kt – e-kmet]/(kme- K) /Vm C M(t) = kmf Ao[ e-Kt – e-kmet]/[Vm(kme- K)] kfm should be km November 2007
(B) Drug Given i.v., Metabolite Formed in the Body • When K > Km, M terminal phase kinetics follows its own profile • When Km > K, M terminal phase kinetics follows the parent drug profile • The slowest step is rate-limiting • M T1/2 can’t be shorter than T1/2 of the parent drug km should be kme November 2007
Metabolite Conc. versus Time Profile (A) Metabolite is given i.v. CM =DoseMetab i.v.e-Km (B) Drug is given i.v. , metabolite is formed in the body kmfDoseDrug i.v. VM(K-kme) CM = (e(-kmet) - e(-Kt) ) K > kme or kmfDoseDrug i.v VM(kme-K) CM =(e(-kmet) - e(-Kt) ) kme >K Note: Different Mol.Wt of parent drug and metabolite! Use MOLAR doses or correction to calculate CM: Dose Drug i.v. x (Mol.Wt.Met/Mol.Wt.Drug) November 2007 kfm should be km
Metabolite Conc. versus Time Profile Drug is given i.v. , the metabolite is formed in the body K>kme kmfDoseDrug i.v. VM(K-kme) CM = (e(-kmet) - e(-Kt) ) If K >> kme kmfDoseDrug i.v. VM(K-kme) CM = e(-kmet) kme > K kmfDoseDrug i.v VM(kme-K) CM =(e(-kmet) - e(-Kt) ) If kme >>K kmfDoseDrug i.v VM(kme-K) kfm should be km CM =e(-Kt) November 2007
The Impact of kfm on the Metabolite Profile kfm should be km CM and AUC of the metabolite are proportional to kfm November 2007
How to Determine K, kme and kmf ? kfm should be km Knowledge on: • Oral absorption kinetics • Urinary data analysis Step 1: Terminal Phase Step 2: Residual Analysis November 2007
We have two exponents. Do we know which is K or kme? Recall: The slowest step is rate limiting. Terminal slope is “K”. “Residual” slope is kme Terminal slope is kme. “Residual” slope is “K”. November 2007
The Formation Rate Constant kfm and fraction of drug transformed into metabolite CLtot = CLr +CLmet CLmet = CLtot-CLr CLtot =Dose/AUC CLtot =Vd x K CLren = Vd x ke K = ke + kfm CLmet = Vd x kfm fmet=CLmet/CLtot = kfm/K ke Urine D kfm should be km kme M kfm Note: Metabolic Clearance of Drug = Vd x kfm Clearance of Metabolite = Vm x Kmet November 2007
Some drugs, e.g. Moxifloxacin, form more than one metabolite ke Urine Moxifloxacin kmf1 M1 knr kmf2 M2sec M2 Bile kmf = kmf1 + kmf2 +… Kfm should be km Subscript 1 & 2 remain Some metabolites can be further biotransformed to produce secondary and tertiary metabolites. Metabolites can be excreted in urine, in bile, or… November 2007
Mini Quiz • Q1: Drug dose of 250 mg was given I.V. bolus. Mol.Wt. of the drug is 200 Da. The metabolite, conjugate, is formed in the body and its Mol.Wt. is 350 Da. • (a) We would like to calculate Cm in the plasma in ng/mL. What will be the correction factor? • b) We would like to calculate Cm in mM. What should we do? November 2007
Answers (a) • Drug M.Wt. = 200 Da • Metabolite M.Wt =350 Da • Correction= 350/200= 1.75 • Dose 250 mg = 250 000 mg, Vm = x L units mg/L=ng/mL (b) • 200 mg = 1 mmol = 1000 mmol • 250 mg = 1250 mmol • Vm = x L units mM November 2007
Mini Quiz, Cont’d • Q2: Drug t1/2 is 4 h. M1 t1/2 is 1.2 h, and M2 t1/2 is 7h when given I.V. on a separate occasions. What will be t1/2 of M1 and M2 when formed in the body from the parent drug? November 2007
Mini Quiz, Cont’d • Q3: “K” of the drug is 0.25 1/h. One metabolite is formed and kmf is 0.05 1/h. Another drug, the inducer of metabolism, was co-administered and kmf is 0.15 1/h. No change in “K” was observed. What fraction of the dose was metabolized before and following the co-administration of the inducer? November 2007