Corneal Path
Corneal Path. Lecture 08/25/08: Corneal Dystrophies. Arcus Senilis. Elevated Cholesterol See PCP for blood work-up. Arcus Senilis. Hudson Stahli Line. A brown, horizontal line across the lower third of the cornea, occasionally seen in the aged. No Tx. Hudson Stahli Line.

Corneal Path
E N D
Presentation Transcript
Arcus Senilis • Elevated Cholesterol • See PCP for blood work-up
Hudson Stahli Line • A brown, horizontal line across the lower third of the cornea, occasionally seen in the aged. • No Tx
Band Keratopathy • Precipitation of calcium salts on the corneal surface (directly under the epithelium) • Patients with band keratopathy complain of the following: • Decreased vision • Foreign body sensation • Ocular irritation • Redness (occasionally) • Tx: Debridement
Limbal Girdle of Vogt • Very common, bilateral, age-related condition.Corneal degeneration.Clinical features:Symptoms: asymptomatic and requires no therapy.Signs:Crescenteric, white opacities of the peripheral cornea in the interpalpebral zone along the nasal and temporal limbusMay be separated from the limbus by a clear zone or without a clear zone in between
Salzmann’s Nodular Degeneration • Usually following trachoma or phlyctenular keratitis • Characterized by multiple superficial blue white nodules in the midperiphery of the cornea • Medical therapy consists of lubrication, warm compresses, lid hygiene, topical steroids, and/or oral doxycycline
Climatic Droplet Keratopathy • Degenerative condition characterized by the accumulation of translucent material in the superficial corneal stroma • Sector iridectomy, corneal epithelial debridement, lamellar keratoplasty, and penetrating keratoplasty have all been employed in the treatment of visually incapacitating CDK.
Corneal Farinata • Bilateral speckling of the posterior part of the cornealstroma • VA unaffected
Pellucid Marginal Degeneration / Keratoglobus • Bilateral, noninflammatory, peripheral corneal thinning disorder characterized by a peripheral band of thinning of the inferior cornea • Tx: RGPs / Keratoplasty • Surgery needed for Keratoglobus
Lecture 09/08/08 EBMD (Bergmanson) • Keratoconus (continued) • Making the Dx
Fleisher’s Ring Cause: Thickened tear film where lids meet
Hydrops Rupture in Descemet’s membrane
EBMD Epithelial Basement Membrane Dystrophy
Meesmann’s Dystrophy Intraepithelial cysts with amorphous material/cellular debris Tx: usually not needed
Map/ Dot/ Fingerprint Dystrophyaka “Anterior Membrane Dystrophy” BM is laid down abnormally by epithelial cells build up of material Pts > 60 Negative staining
Tx: for EBMD • Lubricant/gtts; ung • Bandage CL • Stromal puncture • Epithelial scraping • PTK
Surgical Tx • PKP (Penetrating) vs. LKP (Lamellar) • Most surgeons tx w/ PKP • Adv of LKP • Not intraocular • Fewer complications • Preserved endothelium • Low risk of rejection • Preserves global strength
Reis-Buckler’s Dystrophy Autosomal dominant dystrophy Characterized by small discrete opacities centrally just under the epithelium which may have a honeycomb pattern ALL is being replaced by reticular material (scar-like tissue)
Inherited Band Keratopathy Tx: Chelating agent EDTA
Stromal Dystrophy • Granular Dystrophy • Lattice Dystrophy • Gelatinous drop-like dystrophy
Bacterial Keratitis -WBCs only found in infectious keratitis. -Acute (24-48 hrs), rapidly progressive corneal destructive process or a chronic process. -Caused by corneal epithelial disruption caused by trauma, contact lens wear, contaminated ocular medications and impaired immune defense mechanisms. -Tx. With Polytrim, Vigamox, and broad spectrum antibiotics
Radial Keratotomy Problems *Refractive surgery procedure to correct mild to moderate degrees of myopia (2 to 5 D). *Incisions can split open making them vulnerable to corneal infections (fungal/bacterial) -If infection happens w/i 24 -48 hrs, bacterial and not fungal. -Tx aggressively with Polytrim, Vigamox, or broad spectrum antibiotics. -F/U in 1 day.
Fungal Keratitis • Feathery Borders, w/ hx of plant/vegetable matter trauma. • Tx w/ prolonged course of systemic and topical anti-fungal (Natamycin), and frequent scrapings or localized debridement to remove necrotized epithelial tissue.
Pseudomonas Keratitis *Pseudomonas can progress fast! Within 24 hours -hypopyon, infiltrates in cornea, KPs, plasmoid aqueous (AC is jello) -pain, decreased VAs, redness
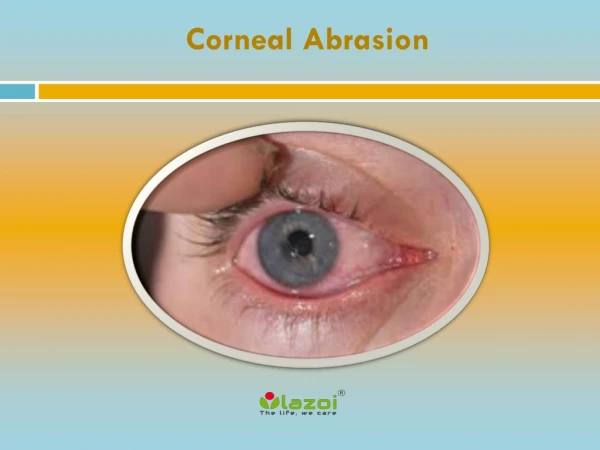
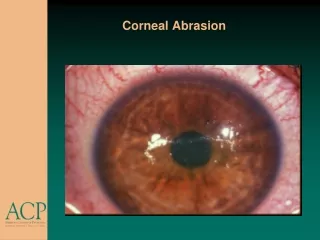
Corneal FB *May develop corneal ulcer. *r/o intraocular FB. *Remove FB, unless removal will cause more damage than leaving it undisturbed. -Topical antibiotics after removal -Topical NSAID (Ketorolac) or short acting cycloplegic for relief of symptoms
Intraocular Foreign Body • *Intraocular FB –passes basement membrane of cornea. • -Improper removal can cause collapsed AC, traumatic glaucoma, endophthalmitis if infected. • *Refer to surgeon.
Traumatic Cataract *Most common complication of non-perforating and perforating injuries to the globe.
Hypermature/Morgagnian Cateract *May me caused by severe trauma. *Liquified cat with intact nucleus inferiorly displaced.
Bollus Keratopathy *Compromised endothelial cell pump mechanism as the endothelial cell density decreased and decompensated; Folds in stroma from stromal edema. *Can be induced by cataract surgery or other trauma. *Manage w/ NaCl 5% gtts and ung; CL for pain; IOP lowering meds; Penetrating Keratoplasty in advanced cases.
RA-associated peripheral ulcerative keratitis *Hx of CT dz. *May cause stromal thinning, descemetocele (only PLL and endothelium left due to corneal thinning) in progressive keratolysis, and perforation. *Promote re-epithelialization by ocular surface lubrication, patching or bandage soft contact lens.
Alkaline Burn *Immediate irrigation of eye until the pH of the cul-de-sac has returned to neutrality. (pH= 7.0) *Prophylactic broad spectrum antibiotic; cycloplegic drops; topical steroids to decrease inflammation; lubrication; soft CL…
Pseudomonas Keratitis Vigamox