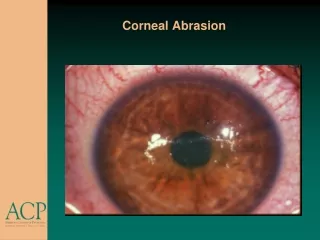
Corneal Transplants
Corneal Transplants. Lecture 15 Liana Al-Labadi, O.D. Corneal Transplantation. The most common form of transplantation With over 2500 grafts in the UK & 32000 grafts undertaken in the US annually Outcomes, including failure & complications of the procedure are well known & depend on

Corneal Transplants
E N D
Presentation Transcript
Corneal Transplants • Lecture 15 • Liana Al-Labadi, O.D.
Corneal Transplantation • The most common form of transplantation • With over 2500 grafts in the UK & 32000 grafts undertaken in the US annually • Outcomes, including failure & complications of the procedure are well known & depend on • Recipient aetiology • Preoperative comorbidity • Health of donor tissue • Modern-day success in transplantation is attributed to: • Eye banking • Storage techniques • Ocular phramacology • Equipment • Modern surgical techniques
Preoperative Risk Factors • Evaluation of Preoperative Risk Factors • Donor factors studied include: • Age • Time from death to enucleation • Preservation time • Endothelial cell count • Recipient factors include: • Age • Indication for transplantation • Prior Grafts • Preoperative ocular conditions (Gluacoma, uveitis, infection, OSD)
Donor Tissue • Recruitment of donor tissue • Donor tissue should be removed within six hours after death • Viable storage period of the removed corneo-scleral button is 7-14 days • Grafts from donors <12months or >70 years are preferably not to be used • Contraindication for donor selection: • Death of unknown cause • Certain infectious diseases of the CNS • Jacob-Creutzfeld, SSPE, Progressive Multifocal Leuko-encephalopathy • Certain systemic infections (AIDS, septicemia, syphilis, viral hepatitis) • Leukemia & disseminated lymphoma • Intrinsic eye diseases (tumors, active inflammation, previous intra-ocular surgery)
Recipient Cornea • Poor prognostic factors: • Absence of corneal sensations • Stromal vascularization • Corneal thinning at the expected recipient-donor margin • Active inflammation
Preoperative Instructions • Preoperative instructions to patients include: • If currently on anticoagulants or any blood thinning medications, continue taking it as prescribed by PCP • If taken for any reason other than prescribed blood thinner, please discontinue using it 7-10 day prior to surgery date • If taking Flomax or Cardura- must discontinue & take atropine instead for 3 days prior to surgery • A prescription for AB drops (Vigamox) must be used 1 day before surgery • Contact lenses must be removed the night prior to the surgery • Nothing to eat or drink or smoke 8 hours prior to surgery- small sips of water is allowed • Continue using systemic medications & glaucoma drops as usual
Following Surgery • Immediately following the surgery: • Patch & shield should not be removed unless instructed by staff/doctor • Pain medications may be prescribed • OTC pain medications (Tylenol, Advil, Aspirin) may be used instead • Patients should continue using all prescription medications (oral & topical) as before surgery
Postoperative Instructions • What To Expect: • Explain drop & follow-up schedule • Explain the need to use drops for the next 3 months • Be certain to shake the bottle thoroughly prior to each drop • Allow 2-3 minutes between each drop to ensure full benefit of each drop • Eye may feel dry or “gritty”: that may last for several weeks • Use preservative free artificial tears • Refrain from rubbing eyes for at least 8 weeks • Eyelids may be mildly “droppy” or swollen: normal & will go away • Vision is blurred • Eye shield at night while sleeping for at least 6-12 weeks
Postoperative Instructions • What To Expect: • Full time eye protection for the 1st 2-3 months & sunglasses to protect against light sensitivity • Can resume most activities in 1 week • No make up x 7 days • No swimming or hot tub x 14 days following surgery • Wear protective eyewear during any contact sports or around small children for a minimum of 3 months • If any symptoms of sudden onset of redness, pain, sensitivity to light, or visual decline occur • Must contact doctor ASAP
Postoperative Care • Careful postoperative care following PK is critical for successful outcome • Slit lamp findings should reveal: • An intact, smooth & well-hydrated corneal epithelium within 7 days • Sutures intact with knot buried • Well centered graft • Clean eyelids & adequate tear film to prevent onset of DES signs & symptoms
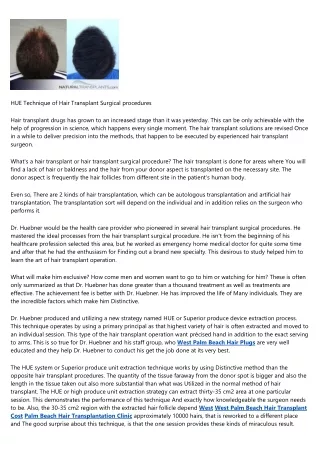
Postoperative Complications • Graft is neurotrophic x 6months & patient will never develop absolute normal sensation - patient will be unaware of impending corneal problems • Graft Rejection • Epithelial defects • Ulceration & corneal infiltrates • Infection • Wound leak- Low IOP is one of the most typical early complications • Uncorrected sphere, cylinder, and HOA errors typically exist postoperatively • Consider suture adjustment as soon as able to measure K astigmatism • Eccentric graft • Tight sutures/ Broken sutures • Endophthalmitis • Glaucoma • Recurrence of initial disease in the donor graft
Ultimate Goal • Ultimate Goal of PK is a clear graft
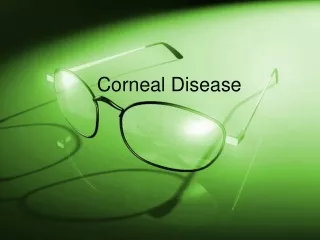
Graft Rejection • Occurs when the donor K doesn’t retain the transparency sufficient for adequate vision • The most common cause is endothelial cell dysfunction but other causes include: • Sub-optimal condition of donor tissue • Intraocular inflammation • Endothelial trauma during surgery • Pre-existing glaucoma • 50% of grafts occur within the first 6 months • The majority occur in the first year post-op
Graft Rejection • Symptoms: • Decreased vision • Mild pain • redness • photophobia • Often asymptomatic & diagnosed on routine follow-up exam
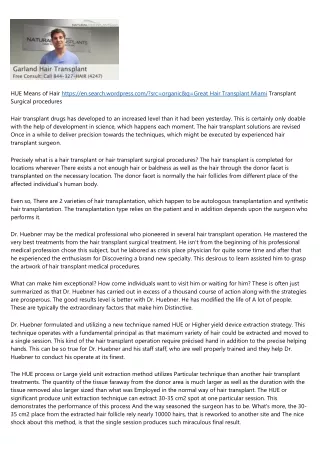
Graft Rejection • Critical Signs: • New keratic precipitates • Endothelial rejection line: A line of KPs on the corneal endothelium • aka Khodadoust line • Stromal edema • Subepithelial infiltrates • An irregularly elevated epithelial line (epithelial rejection line) • Localized stromal vascularization & infiltrates
Graft Rejection • Other signs: • Conjunctival injection- circumcorneal • AC inflammation • Graft vascularization • Broken graft sutures • Usually no discharge present: tearing most likely
Graft Rejection • Work-Up • Case History • Time since PK? • Current meds? • Recent change in steroid regimen? • Indication of PK (i.e. HSV) • Slit Lamp Exam • Careful inspection for the endothelial rejection line, KPs, infltrates
Graft Rejection • Endothelial Rejection Treatment: • Topical Steroids • PF Q1H & steroid ung QHS • Systemic steroid & steroid injections in severe cases • Cyclosporine agent (Restasis BID) • May be helpful in the treatment & prevention of graft rejection
Graft Rejection • Epithelial Rejection Treatment: • Increase steroid drops: double the current level of topical steroids or use PF QID • PF Q1H & steroid ung QHS • Cycloplegic agent • Topical cyclosporin