Download
1 / 20

E N D
Please note, these are the actual video-recorded proceedings from the live CME event and may include the use of trade names and other raw, unedited content. Select slides from the original presentation are omitted where Research To Practice was unable to obtain permission from the publication source and/or author. Links to view the actual reference materials have been provided for your use in place of any omitted slides.
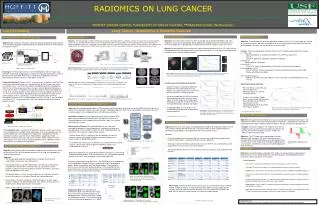
Lung-Cancer Screening Pros and Cons Alan Sandler, MD Oregon Health & Science University
Background • 94 million current or former smokers remain at risk for development of lung cancer in U.S. • Randomized trials examining use of CXR with or without sputum cytology revealed no reduction in mortality • Several observational studies using low dose helical CT scans detect more nodules and lung cancers, including early stage lung cancers (Doria-Rose, et al Screening and Prevention of Lung Cancer. Lung Cancer: A Multidisciplinary Approach to Diagnosis and Management 2010) NLCSTR Team NEJM 2011
Backgroundcont. • The NLST, a randomized trial of screening with the use of low-dose CT as compared with screening with the use of chest radiography • Participants were enrolled from August 2002 through April 2004; screening took place from August 2002 through September 2007. Participants were followed for events that occurred through December 31, 2009 • A total of 53,454 persons were enrolled; 26,722 were randomly assigned to screening with low-dose CT and 26,732 to screening with chest radiography
Inclusion Criteria • Age - 55 to 74 years of age • History of cigarette smoking of at least 30 pack-years • Former smokers must have quit within the previous 15 years
Exclusion Criteria • Persons who had previously received a diagnosis of lung cancer • Chest CT within 18 months before enrollment • H/o hemoptysis, or unexplained weight loss of more than 6.8 kg (15 lb) in the preceding year
Selected Baseline Characteristics of the Study Participants. The National Lung Screening Trial Research Team. N Engl J Med 2011;365:395-409.
Results of Three Rounds of Screening. The National Lung Screening Trial Research Team. N Engl J Med 2011;365:395-409.
Diagnostic Follow-up of Positive Screening Results in the Three Screening Rounds. The National Lung Screening Trial Research Team. N Engl J Med 2011;365:395-409.
Complications after the Most Invasive Screening-Related Diagnostic Evaluation Procedure, According to Lung-Cancer Status. The National Lung Screening Trial Research Team. N Engl J Med 2011;365:395-409.
Stage and Histologic Type of Lung Cancers in the Two Screening Groups, According to the Result of Screening. The National Lung Screening Trial Research Team. N Engl J Med 2011;365:395-409.
Cumulative number of lung cancers was higher with low-dose CT screening • 20% reduction in the incidence of dying from lung cancer (low-dose CT versus chest radiograph) • Deaths from lung cancer again favoring the low-dose CT group Cumulative Numbers of Lung Cancers and of Deaths from Lung Cancer N Engl J Med 2011; 365:395-409
Histologic Type of Lung Cancers in the Two Screening Groups, According to Tumor Stage. The National Lung Screening Trial Research Team. N Engl J Med 2011;365:395-409.
Cause of Death on the Death Certificate, According to Screening Group. The National Lung Screening Trial Research Team. N Engl J Med 2011;365:395-409.
Pros • Reduced mortality • More likely to be early stage and less likely to be late stage than were those discovered after chest radiography. • 20% reduction in lung cancer–specific deaths in the LDCT group • 247 deaths from lung cancer per 100,000 person-years of follow-up after screening with low-dose CT and 309 per 100,000 person-years after screening with chest radiography.
Cons • Is it applicable to the general community? • Diagnostic W/U in community but interpretation of CT scan at screening center • Low dose CT scans used • Trial participants younger with higher level of education better compliance? • Overdiagnosis - test detects a cancer that would otherwise have remained occult • Is it cost effective? • 7 million U.S. adults meet the entry criteria for the NLST, and an estimated 94 million U.S. adults are current or former smokers. • PSA screening and mammography still suffer controversy • Compared with < $5000 per quality-adjusted life-year estimated to implement the clinical practice guidelines on smoking cessation from the Agency for Healthcare Research and Quality
Cause of Death on the Death Certificate, According to Screening Group. The National Lung Screening Trial Research Team. N Engl J Med 2011;365:395-409.
Sunday, February 12, 2012Hollywood, Florida Co-Chairs Rogerio C Lilenbaum, MD Mark A Socinski, MD Co-Chair and Moderator Neil Love, MD Faculty Walter J Curran Jr, MD David Jablons, MD Mark G Kris, MD Suresh Ramalingam, MD Alan B Sandler, MD