Download
1 / 13
130 likes | 282 Vues
A Decade of Outcomes-Based Drug Coverage in British Columbia. Steve Morgan, Ken Bassett, Barbara Mintzes, and Jim Wright University of British Columbia. T H E C O M M O N W E A L T H F U N D. Context: BC. British Columbia 4.1 million residents (3 rd largest province)

E N D
A Decade of Outcomes-BasedDrug Coverage in British Columbia Steve Morgan, Ken Bassett, Barbara Mintzes, and Jim Wright University of British Columbia T H EC O M M O N W E A L T H F U N D
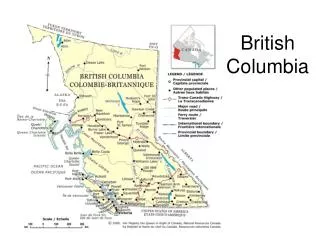
Context: BC • British Columbia • 4.1 million residents (3rd largest province) • ‘Domestic’ Rx Industry generic & biotech • Health Coverage • Universal, public insurance for medical and hospital care • Rx Coverage: • Mix of private/public/uninsured
Context: BC PharmaCare • Tax-financed public drug benefit plan • PharmaCare covered • Social Assistance Recipients • All Seniors • Residents with catastrophic costs • Residents with specific diseases (HIV, Cancer…)
Context: Cost Crises of 80s and 90s Source: CIHI and Statistics Canada
How Cost Crisis Played Out in BC • 1993 review of PharmaCare • Appointment of new Executive Director • Management aware of: • Cost-sharing research from US • Cost-impact research done locally • Decision: • Limit subsidy based on evidence • Establish process to review evidence
The Therapeutics Initiative • Multi-disciplinary group at UBC • Supported by 5-year grant from Ministry • Small core staff • Mandate: • review all products for listing • promote rational drug therapy • advisors to Ministry staff
Genesis of Coverage Framework • 1994 review of nitrate drugs • $3.8M/yr spent on one SR product • Cost 10 times per dose as alternatives • no evidence to distinguish SR efficacy, effectiveness, compliance, or side effects • Manufacturer Criticisms • Failed • Engage partners in dialogue
Evidence Standards • Evidence of high standard • Blinded RCTs • Comparative • Published • Outcomes approach • Total morbidity/mortality impact • ADRs = part of outcomes • Surrogates must be rationalized • Amenities must yield outcome benefit
Implementing Framework • Reference Drug Program • Applied reference based subsidy to 7 classes • Regular reviews for new evidence of comparative “outcome advantages” • Generous exemptions + market freedom • Rigorously Assessed • Data provided to external research teams • Savings > $12M annually
HigherCost Worse Outcomes Better Outcomes LowerCost Simple Econ of Outcomes Approach AvoidWaste Tough Choices Promote Savings Tough Choices
Key Ingredients • Leadership: committed to EBDM • Communication: ongoing, two-way • Credibility: standards of evidence and standing of advisors • Transparency: Communicating process, evidence, and rationale avoids backlash • Necessity…