Download
1 / 21
210 likes | 271 Vues
Learn about retrospective and prospective cohort studies, comparing exposed vs. unexposed cohorts in health research, influencing factors, control measures, and radiation protection in the workplace.

E N D
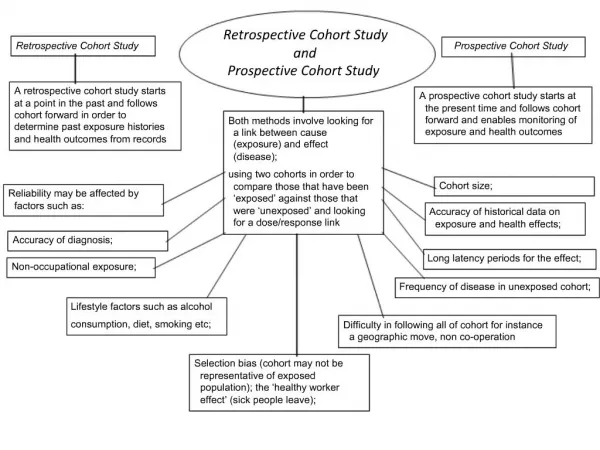
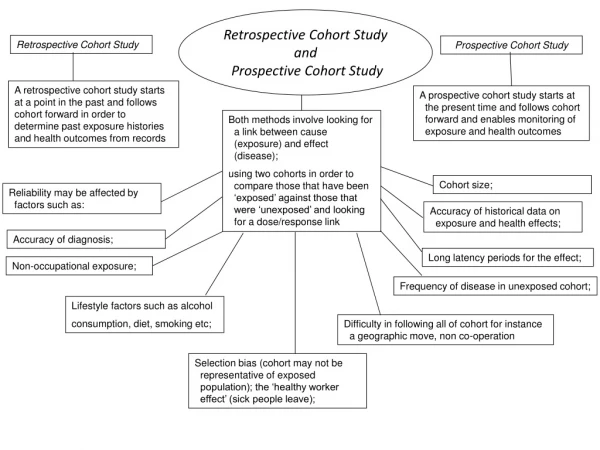
Retrospective Cohort Study and Prospective Cohort Study Retrospective Cohort Study Prospective Cohort Study Aretrospective cohort study starts at a point in the past and follows cohort forward in order to determine past exposure histories and health outcomes from records Aprospective cohort study starts at the present time and follows cohort forward and enables monitoring of exposure and health outcomes Both methods involve looking for a link between cause (exposure) and effect (disease); using two cohorts in order to compare those that have been ‘exposed’ against those that were ‘unexposed’ and looking for a dose/response link Cohort size; Reliability may be affected by factors such as: Accuracy of historical data on exposure and health effects; Accuracy of diagnosis; Long latency periods for the effect; Non-occupational exposure; Frequency of disease in unexposed cohort; Lifestyle factors such as alcohol consumption, diet, smoking etc; Difficulty in following all of cohort for instance a geographic move, non co-operation Selection bias (cohort may not be representative of exposed population); the ‘healthy worker effect’ (sick people leave);
Controls Nature and properties Maximise distance from source and minimise amount of time employees exposed since effect of exposure is dose dependant. Specific doses stated in Ionising Radiation Regulations for classified workers. Likely to receive doses over 6 mSv a year. Non particulate electromagnetic radiation • Artificially generated, normally by the use of electrical energy and emitted when a machine is switched on. Over exposure to be investigated and reported to enforcement authority. X- Rays Can travel a few metres in air, present an external radiation hazard for an individual in the same room or space. Monitoring of staff overseen by a Radiation Protection Supervisor, records kept for fifty years or until person they refer to has reached seventy five years of age. • Can penetrate much further into body but can be shielded with lead or concrete. Monitored by use of personal devices such as film badges or thermoluminescent dosimeters (tld’s). These should then be processed by an approved dosimetry service and results checked against specified regs.
Controls Nature and properties Maximise distance from source and minimise amount of time employees exposed since effect of exposure is dose dependant. Type of ionising radiation formed as a result of radioactive decay. The source should be shielded or contained in a sealed unit or container and where possible the work undertaken in a glove box or fume cupboard to minimise chance of ingestion, inhalation or absorption. Consists of two protons and neutrons (ie a Helium nucleus) Alpha Particles • Travel for only a few centimetres through air • Can be stopped by skin or paper Equipment and surfaces should be decontaminated following work with the particles. Taking of food and drink should not be allowed in areas where the particles are likely to be present. • Ensure all wounds cuts and grazes are covered and protected. • More hazardous if source is taken into body • Use of a Radiation protection adviser / supervisor. • Surveillance
Controls Nature and properties Maximise distance from source and minimise amount of time employees exposed since effect of exposure is dose dependant. Type of ionising radiation formed as a result of radioactive decay. The source should be shielded or contained in a sealed unit or container and where possible the work undertaken in a glove box or fume cupboard to minimise chance of ingestion, inhalation or absorption. Consists of two protons and neutrons (ie a Helium nucleus) Beta Particles Longer range than Alpha Particles Low energy can be stopped by skin High energy can penetrate soft tissue to a depth of over 1cm. Equipment and surfaces should be decontaminated following work with the particles. Taking of food and drink should not be allowed in areas where the particles are likely to be present. • Ensure all wounds cuts and grazes are covered and protected. • More hazardous if source is taken into body, but not as intense as Alpha particles. • Use of a Radiation protection adviser / supervisor. • Surveillance
Occupational Health • Practitioners • Ergonomists • Toxicologists • Epidemiologist • Occupational Hygienists • Occupational Health physicians • Occupational Health nurses • Occupational Psychologists • Radiation Protection Advisers / supervisors / health physicists. • Information from • EMAS - (Employment Medical Advisory Service) • THOR - The Health and Occupational Reporting Network • Industrial Injuries Disabled Board • HSE fatality statistics • RIMEC • Recognition / Identification • Measurement • Evaluation • Control
Structure of the Skin • blood vessels - Tubes that carry blood as it circulates. Arteries bring oxygenated blood from the heart and lungs; veins return oxygen-depleted blood back to the heart and lungs.Sebaceous gland - a small, sack-shaped gland that releases oily (fatty) liquids onto the hair follicle (the oil lubricated and softens the skin). These glands are located in the dermis, usually next to hair follicles. • Sweat gland - a tube-shaped gland that produces perspiration (sweat). The gland is located in the epidermis; it releases sweat onto the skin. • hair follicle - a tube-shaped sheath that surrounds the part of the hair that is under the skin. It is located in the epidermis and the dermis. The hair is nourished by the follicle at its base (this is also where the hair grows). • Heat and Cold receptors- Detect heat and cold and pass info via nerves to central nervous system. • Epidermis - the outer layer of the skin. • Dermis - the layer of the skin just beneath the epidermis. • Subcutaneous tissue - fatty tissue located under the dermis
The Human Ear • Pinna - (also called the auricle) the visible part of the outer ear. It collects sound and directs it into the outer ear canal. • Outer ear canal - the tube through which sound travels to the eardrum. Oval Window- link between stirrup and cochlea. Semicircular canals - three loops of fluid-filled tubes that are attached to the cochlea in the inner ear. They help us maintain our sense of balance. Cochlea - a spiral-shaped, fluid-filled inner ear structure; it is lined with cilia (tiny hairs) that move when vibrated and cause a nerve impulse to form. Auditory nerve - this carries electro-chemical signals from the inner ear (the cochlea) to the brain. Eustachian tube - a tube that connects the middle ear to the back of the nose; it equalizes the pressure between the middle ear and the air outside. When you "pop" your ears as you change altitude (going up a mountain or in an airplane), you are equalizing the air pressure in your middle ear. Hammer - (also called the malleus) a tiny bone that passes vibrations from the eardrum to the anvil. Anvil - (also called the incus) a tiny bone that passes vibrations from the hammer to the stirrup. Stirrup - (also called the stapes) a tiny, U-shaped bone that passes vibrations from the stirrup to the cochlea. This is the smallest bone in the human body. Eardrum - (also called the tympanic membrane) a thin membrane that vibrates when sound waves reach it.
LD50 and LC50 • LC50 (lethal concentration, 50%) or LCt50 (lethal concentration & time) Inhaled concentration of an agent required to kill half the members of a tested population after a specified test period. • Measured in ppm (parts per million )or grams / milligrams per cubic metre of air. • No account is taken of bodyweight in this measurement. • LD50 In toxicology, the median lethal dose, (abbreviation for “lethal dose, 50%”), relates to a single oral dose) of an agent required to kill half the members of a tested population. • Since it is oral dose it is measured in grams or mg per Kilogram body weight. • NOAEL – No Observed Adverse Effect Level • Exposure level at which there are no statistically or biologically significant increases in the frequency or severity of adverse effects between the exposed population and its appropriate control; some effects may be produced at this level, but they are not considered as adverse. • LOAEL - Low Observed Adverse Effect Level • lowest concentration or amount of a substance found by experiment or observation that causes an adverse alteration of morphology, function, capacity, growth, development, or lifespan of a target organism distinguished from normal organisms of the same species under defined conditions of exposure. • Limitations • Ethics / Public opinion • Costly and time consuming • Dose response varies. • May not display synergistic effects that may arise in humans exposed to other agents at the same time. • Difficulty with no observed effects level for carcinogens. • There can be wide variability between species as well; what is relatively safe for rats may very well be extremely toxic for humans, and vice versa. • For example, chocolate, harmless to humans, is known to be toxic to many animals. • Advantages • Avoids human exposure. • Data can be collected more quickly than for epidemiological studies. • Animals provide good models due to their close genomic relation to humans. • More likely to show carcinogenic potential than in-vitro tests such as the Ames test.
Risk assessment Reg 6 • Requires that an employer not carry out work liable to expose employees and non Employees to a substance hazardous to health without a risk assessment and implementation of the steps necessary to comply with the regulations. • Theassessment must include consideration of any information provided by the supplier of a substance (CHIP) • Must be reviewed regularly, and also when there is reason to think the assessment is no longer valid, if the system of work is changed • Because of the results of health Monitoring. The assessment must also consider any occupational exposure limit, in particular, those mandated by the HSE. • Accidents, incidents and emergencies • Reg 13 • Requires that employers prepare for possible accidents, incidents and emergencies involving hazardous substances by: • Preparing emergency procedures, including provision of First Aid; • Making available technical information on possible accidents and hazards and bringing it to the attention of the emergency services; and • Installing alarms and other warnings and communication systems COSHH as Amended Prevention or control of exposure Reg 7 Requires that an employer prevent exposure to hazardous substances or, if this is not reasonably practicable, that he adequately controls exposure. • Information, instruction and training Reg 12 • Demands that all employees liable to • exposure to hazardous substances are • provided with suitable and sufficient • information, instruction and training, Use of control measures Reg 8 Employers must take all reasonable steps to ensure that control measures, and any necessary equipment of facilities, are properly used or applied. Employees must use the control measures properly, return them after use and report any defective equipment. • Health surveillance Reg 11 • Requires that health surveillance of employees is carried out where: • An identifiable disease or adverse health effect may be related to the exposure; • There is a "reasonable likelihood" that the disease or health effect may occur under the particular conditions of work; • Valid techniques exist for detecting indications of the disease of health effect; and The technique presents a low risk to the employee; • where there is exposure to certain substances in specified occupations: • Monitoring Exposure Reg 10 • Where the risk assessment indicates that workplace monitoring of exposure is necessary, the employer must perform such monitoring • unless he can demonstrate another means of preventing or controlling exposure • Monitoring must be at regular intervals in addition to when a change occurs that may affect exposure Maintenance and testing of control measures Reg 9 Requires that employers maintain control measures in efficient working order and in good repair
6 – Risk assessment 7 – Prevention or control of Exposure. (Adequate control) Principles of good practice Schedule 2 of Reg 7 8 – Use of control measures Design process to minimise ex. Route of exposure. Controls proportionate to risk Escape of substance minimised PPE in addition Review effectiveness Info., training and instruction Higher risk – do not introduce. 9 – Maintenance and testing of control measures COSHH amended L5 10 – Monitoring exposure 11 – Health Surveillance - Schedule 6 - Benzene – Manufacturing process 12 – Information, instruction and training 13 – Accidents, incidents and emergencies
Zoonoses are animal infections which may be transmitted to people in the course of their work. Common examples include: • Anthrax • Brucellosis • Orf • Glanders Controls • Anthrax is an acute infectious disease of farm animals caused by a bacterium • Transmitted to man by contact with infected hair, hides, excrement or products such as bonemeal • Fatal without treatment • Initial lesion rapidly becomes ulcerated • Treatment is by penicillin • Inhaling the pathogen causes pulmonary anthrax which is usually fatal in 3 or 4 days • First stage of control strategy is to • assess those people at risk Factors to • consider include: • Work being carried out • Susceptibility to infection of the workers • How infections might occur • How likely exposure to infection is. • Most common route of entry is via the skin, by way of open cuts, sores or abrasions which provide direct entry to blood stream, • inhalation of contaminated dusts, • Contact with conjunctiva of eyes, • Direct injection by cuts from infected animals or animal bites • Direct ingestion via hands • Brucellosis caused by the bacterium Brucellaabortus, which may infect people handling cattle or pigs or their carcasses in abattoirs • Not very severe but involves loss of appetite, headache, insomnia and slight fever • In the UK a policy of eradication has been pursued since the 60’s by destroying any infected cattle Zoonoses • Where animal products likely to emit infected dust are handled (e.g. wool, skin, hides, pelts), LEV and possibly RPE should be provided to prevent airborne infection • Specific immunisation of workers may be necessary • Clean & hygienic animal living conditions and disinfection of stalls will also ensure better hygiene in factory premises and will reduce probability of infection • Orf is a contagious pustular dermatitis of viral origin, mainly affecting farm workers, shepherds, sheep shearers, butchers and abattoir workers • Lesion enlarges and often becomes ulcerated, exuding fluid and pus • Complete recovery occurs in about 3 weeks • Automation to reduce human contact and enclosure of aerosol-producing activities will reduce exposure to infection • Finally, medical checks, training and information, procedures, instruction and records will give added protection to workers • Glandersis an infectious disease of horses, donkeys and mules caused by the pathogen Pseudomonas mallei • Transmitted to humans by nasal or mouth secretions from the infected animal • Abscesses appear on hands, arms or face • Lasts up to 4 months but is treatable with modern antibiotics
Aids • Acquired Immune Deficiency Syndrome Caused by Human Immunodeficiency Virus (HIV), which attacks the immune system • Virus is found in most body fluids but is delicate and relatively easy to kill with heat and chemicals • It has low infectivity and transmission is thought to be more likely with repeated exposure to infection rather than to a single contact • Occupational risk comes from accidental inoculation or contamination of a cut or abrasion with blood or body fluids of an infected person • Doctors, nurses, dentists, laboratory and hospital staff are at some risk, since they may come into close contact with body fluids • Other workers possibly at risk might include community, welfare, custodial and emergency service workers and first aiders • Hepatitis • Those at risk include doctors, surgeons, nurses and porters • Infection amongst health workers is a result of contact with blood or excreta of patients suffering from viral hepatitis or in whom the disease is still in its incubation stage • Porters and refuse disposal are at risk from carelessly discarded syringes and other sharps - the problem is becoming worse with the increase in drug addiction Aids and Hepatitis • Course of disease is similar to Weil’s Disease, but is usually much less severe and normally self-limiting with recovery in about 6 weeks • In about 5% of cases, chronic infectious hepatitis follows, leading to cirrhosis and possibly death • Persons exposed to risk can be protected with injections of gammaglobulin • In all cases, protective disposable gloves should be worn and hands and arms washed regularly with disinfectant • Many of the precautions taken against other infections, especially Hepatitis B, will be equally effective against HIV. They include: • Prevention of puncture wounds, cuts and abrasions in the presence of blood and body fluids; • Protection of existing wounds and skin lesions • Control of surface contamination by containment and disinfection • Safe disposal of contaminated waste, especially sharps
Support – this includes the encouragement, sponsorship and resources provided by the organisation, line management and colleagues. Demands– this includes issues such as workload, work patterns and the work environment. HSE Stress Management Hazards • Relationships – this includes promoting positive working to avoid conflict and dealing with unacceptable behaviour. Control– how much say the person has in the way they do their work. • Role – whether people understand their role within the organisation and whether the organisation ensures that they do not have conflicting roles. Change– how organisational change(large or small) is managed and communicated in the organisation
Pre-employment screening And on-going surveillance Cold Stress – Difficulty in controlling core body temp. Provision and wearing of thermal clothing, footwear undergarment ,high CLO rating Reduction in heart rate Monitor activity level, to generate some heat but not to sweat. Breaks with warm rest area. Persistent shivering with blue fingers and lips Cold Stress Mental impairment with stress No possibility of being locked in, ability to open from inside Regular maintenance and alarm to detect leaking refrigerant Hypothermia and frost bite which is inflammation of the skin and tissue damage. Training on hazards involved with cold working Chillblains causing redness, tingling and pain in the affected area.
Controls in Garage Physiological Effects Carbon monoxide absorbed via the lungs into bloodstream, displaces Oxygen by chemically bonding to the Haemoglobin. Reducing oxygen carrying capacity of blood and therefore supply to tissues. Minimising duration of engine running time. Local exhaust ventilation attached to hose pipes as well as good ventilation to workshop and pits. Carbon Monoxide CO only slowly displaced from body. Regular maintenance of LEV system and fitting CO alarms Causes drowsiness, headaches, skin colour changes (blue lips), dizziness breathlessness, unconsciousness and death above 5% Specific CO hazard training to employees . Segregating area from customers
Main Function and factors to consider Regulations • Regulation 3 • Duty of employer to make provision for first aid. • Assessment of need • First –aid materials, eqpt and facilities • First-aid personnel Preservation of life and minimisation of the consequences of injury until medical help is obtained, and treatment of minor injuries. Health and Safety (First-Aid) Regulations 1981 Number, composition and distribution of workforce. • Regulation 4 • Duty of employer to provide information to employees on first-aid Hazard and level of risk present and past accidents. • Regulation 5 • Self employed duty to provide first-aid eqpt • Duties of self employed Distance from medical facilities Number of first-aiders and level of training as well as cover for shifts, leave and sickness
Factors to consider and control measures Health effects Control of Asbestos at Work regs 2012 Mesothelioma A form of cancer that affects the external lining of the lung or the peritoneum. Long latency period and almost always terminal • RA – to contain • Type of asbestos • Likely to become airborne and in what concentration. Asbestosis Form of pneumoconiosis –lung fibrosis. Scarring and inflammation of the lung tissue. Irreversible, chest pain, fatigue laboured breathing Asbestos Limit number of people exposed Limit contamination spread. Limit fibre emission at source (work methods) Diffuse pleural thickening Non- Cancerous Causes thickening of the tissue which makes it less able to expand during breathing Licencing and Training on removal Cancer of the bronchus Malignant growth within bronchus of lung, terminal Use of specific PPE
Exposure limit value – 87dB Upper exposure action value – 85dB Lower exposure action value – 80dB L108 - Controlling noise at work Noise survey and Eqpt. Information to gather Personal noise monitoring and frequency analysis Review of previous surveys Basic survey followed by a more detailed survey Consultation Competent assessor eqpt calibrated before and after measurements Use results to plot noise map for area. Assessment of current controls Legal requirements and limits Control of Noise at Work R. 2005 Basic Survey Simple sound level meter for spot checks and integrating sound level meters. Measure at planned points to ID exposures at action levels. Noting machinery in operation at time. Site layout and location of machines. Number and location of workers and audiometry records Shift times and patterns with likely duration of exposure • Detailed Survey • Integrating sound level meters • Appropriate sample times to measure Leq (equivalent continuous sound level), use nonogram to calculate exposure LEPw, LEPd • Measurement of peak noise levels and plotted on noise map. • Use of frequency analysis useful to decide on controls such as enclosure • Personal noise exposure using dosimeter or microphone close to ear • Selection of hearing PPE with suitable SNR (Single Number Rating) Identify noisy machines and review maintenance records for identification purposes. Manufacturers data
Reasons for Introduction and Difficulties Signs Sudden mood changes Safety critical posts. Following accident or incident. Part of rehabilitation stage following discovery of use. Pre-employment. Becoming confused Abnormal fluctuations in concentration and energy levels General statement of aims. Responsibilities. Definition of drug misuse. Rules that will apply. Notification of prescribed drugs. Reporting suspicions. Procedure following failed test. Support and help available. How to return following Treatment. Drug and Alcohol Abuse Impaired job performance / more accidents Poor time keeping and more short term sickness Deterioration in relationship with colleagues Dishonesty or theft Union agreement – staff trust Data protection Cost – lab, competent tester False positives / Unexpected results of alcohol or presence of drugs paraphernalia Change in appearance, scruffy or needle marks, slurred speech.
Measuring Instruments Black globe thermometer - Radiant Temperature Dry bulb thermometer– Normal air temp. Wet bulb thermometer - covered in muslin sleeve (found in psychrometer. ) Wet bulb Thermomter Index Used for heat stress. Sorbent tube – full of adsorbent e.g. charcoal. Cellulose filter paper, Acetone bath. Cowl Dry weight filter paper – Cyclone head - Respirable Simple sound level meter Integrated sound level meter Octave band frequency analysis Measuring Instruments Humidity – Hygrometer (psychrometer) Combination of wet and dry bulb thermometers. Vane anemometer – Wind speed Kata Thermometer – low wind speed Wet bulb globe temperature index To measure heat stress. Smoke tube Manometer –Pressure differentials PitotTube – Static pressure or velocity by using calculation Thermal or hot wire anemometer – air velocity Accelerometer – Measures vibration
Regulations Control of Noise at Work Regs 2005 Exposure limit value – 87dB Upper exposure action value – 85dB Lower exposure action value – 80dB L108 - Controlling noise at work Health and Safety (First-Aid) Regulations 1981 Management of Health and Safety at Work regs1999 Workplace Health safety and Welfare regs 1992 Manual Handling Operations regs 1992 L23 Personal Protective Eqptregs 1992 Health and Safety (DSE) regs 1992 PUWER 1998 Control of Artificial Optical Radiation at Work regs 2010 Ionising Radiation regs1999 Radiation Protection Adviser Radiation Protection Supervisor COSHH 2002 as Amended L5 Legionella L8 Control of Lead at Work Regs 2002 L132 Control of Asbestos at Work Regs 2012 Control of Vibration at Work Regs 2005 (L140 HAVs) Exposure action value of 2.5 m/s2 A(8) at which level employers should introduce technical and organisational measures to reduce exposure. Exposure limit value of 5.0 m/s2 A(8) which should not be exceeded