HYPOKALEMIA
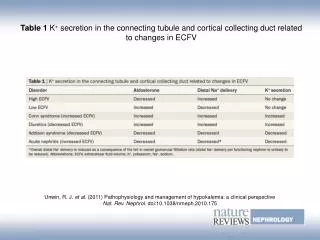
HYPOKALEMIA. Definition. serum potassium concentration < 3.5 mEq /L Etiology total body potassium deficit Poor intake Excessive renal & GI loss serum potassium is shifted into the intracellular compartment drug. Drug induce hypo K. Category & Clinical presentation.

HYPOKALEMIA
E N D
Presentation Transcript
Definition • serum potassium concentration < 3.5 mEq/L Etiology • total body potassium deficit • Poor intake • Excessive renal & GI loss • serum potassium is shifted into the intracellular compartment • drug
Category & Clinical presentation ECG changes: ST-segment depression or flattening,T-wave inversion, and U-wave elevation
Treatment • K supplement 3 salt (Chloride, phosphate, carbonate) • PO mild to moderate (should be divided into 3-4 doses to minimize the developement of GI side effects) • IV severe (K < 2.5 mEq/L) exhibiting signs symptoms of hypokalemia patients unable to tolerate oral therapy
KCl oral • 10% KCl elixir (20 mEq/15 ml) • Ped KCl 2% (4 mEq/15ml)
KCl IV infusion • NaCl • D5W advoided • 10 to 20 mEq of potassium is diluted in 100 mL 0.9% NaCl • administered through a peripheral vein over 1 hour • Mutiple dose: can be repeated as needed until the serum potassium concentration normalizes (equilibium time 30 min)
KCl IV infusion (Conc.) • Severe K depletion • KCl 300 to 400 mEq/day • dilute 40 to 60 mEq in 1,000 mL 0.45% NaCl • Rate of infusion: not exceeding 40 mEq/h • Central intravenous line into a large vein (e.g., superior vena cava)
Alternative therapy Potassium-sparing diuretics • Spironolactone : 25-mg, 50-mg, and 100-mg tablets • Start 25 to 50 mg daily titrated to a maximum dose of 400 mg/day. • side effects: hyperkalemia, gynecomastia, breast tenderness, and impotence
Alternative therapy • Triamterene: 50-mg and 100-mg capsules • Start 50 mg twice daily titrated to 100 mg twice daily • side effects: hyperkalemia, sodium depletion, and metabolic acidosis • Amiloride: 5-mg tablet • Start 5 mg daily; however, 10 mg can be given in those with severe hypokalemia
Alternative therapy • Generally, concomitant use of potassium supplementation with potassium-sparing diuretics is not necessary. • There is a significant risk of hyperkalemia during combination therapy, especially in patients with underlying renal insufficiency or diabetes mellitus.