HYPOKALEMIA
HYPOKALEMIA. Salient Features. 55 y/o male Diarrhea for several weeks to admission 3 days PTA: progressive weakness. Laboratory Findings:. Chemistry Profile. Laboratory Findings:. Arterial Blood Gas Profile: Urine Potassium: 15 meq/L (NV: usually >15 meq/L). Guide Questions:.

HYPOKALEMIA
E N D
Presentation Transcript
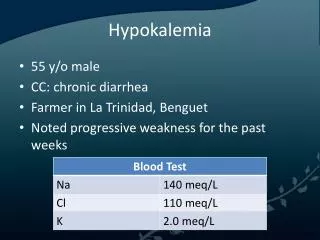
Salient Features • 55 y/o male • Diarrhea for several weeks to admission • 3 days PTA: progressive weakness
Laboratory Findings: Chemistry Profile
Laboratory Findings: Arterial Blood Gas Profile: Urine Potassium: 15 meq/L (NV: usually >15 meq/L)
Guide Questions: 1.) Using an algorithm, discuss the diagnostic approach to hypokalemia. What is the cause of hypokalemia in this patient?
DIAGNOSTIC APPROACH TO HYPOKALEMIA Urinary K+ Loss <15 moml/d >15 mmol/d Assess Acid-Base status Assess K+ secretion Metabolic acidosis Metabolic alkalosis TTKG >4 TTKG <2 Acid-Base status Na+ wasting Nephropathy Osmotic diuresis Diuretic Lower GIT K+ loss Remote diuretic use Remote vomiting K+ loss via sweat Metabolic acidosis Metabolic alkalosis Hypertension Diabetic ketoacidosis Proximal Type 2 RTA Distal Type 1 RTA Amphotericin B Vomiting Bartter’s syndrome Hypomagnesemia Mineralocorticoid excess Liddle’s syndrome Harrison’s Principles of Internal Medicine 16th ed. Vol.I, p.260
Causes of Hypokalemia Redistribution into Cells Decrease Intake Increase Loss • Nonrenal • Renal
Causes of Hypokalemia I. Decreased intake A. Starvation B. Clay Ingestion II. Redistribution into Cells A. Acid-Base (Metabolic Alkalosis) B. Hormonal (Insulin, Beta agonist, Alpha antagonist) C. Anabolic State (folic acid) D. Other (Hypothermia, Pseudohypokalemia)
Causes of Hypokalemia III. Increased Loss A. Nonrenal 1. Gastrointestinal Los (diarrhea) 2. Integumentary Loss (sweat) B. Renal
Cause of Hypokalemia in the patient: • Gastrointestinal lossesdiarrhea (secretory) • Urine potassium level less than 20 mEq/L suggests gastrointestinal loss • Stool has a relatively high potassium content, and fecal potassium losses could exceed 100 mEq per day with severe diarrhea.
Gastrointestinal Loss • Hypokalemia is also due to increased K+ renal excretion • Loss of Gastric contents results in volume depletion and metabolic alkalosis, both of which promotes kaliuresis
Gastrointestinal Loss • Stimulates aldosterone release=augments K+ secretion by principal cells • There is an increase in distal delivery of NaHCO3 which enchances the electrochemical gradient favoring potassium loss in urine.
SIGNS & SYMPTOMS • Fatigue • Myalgia • Muscular weakness & paralysis • Hyporeflexia • Dyspnea • Arrhythmia • Predispose to digitalis toxicity • Constipation
SIGNS & SYMPTOMS • Risk of hyponatremia • resultant confusion, headaches, & seizures • Irritable • Nervousness • anorexia • Ileus
Adverse Medical Implications • Muscle weakness and paralysis (more negative resting membrane potential) • Respiratory • Hypoventilation (due to respiratory muscle weakness or paralysis) • Gastrointestinal • Paralytic ileus
Adverse Medical Implications • Cardiac • ECG changes • Due to delayed ventricular repolarization • Early changes: flattening or inversion of T wave, prominent U wave, ST-segment depression, prolonged QU interval • Severe K+ depletion: prolonged PR interval, decreased voltage and widening of QRS complex
A: Normal B: flattening of T wave C-F:U wave, ST-depression, prolonged QU interval
Adverse Medical Implications • Cardiac • Increased risk for ventricular arrythmias • Potential digitalis toxicity • Risk for Hypertension • Exercising skeletal muscle insufficient blood flow increased risk for rhabdomyolysis • Metabolic acidosis (due to increased bicarbonate excretion)
Adverse Medical Implications • Renal • Risk for renal cystic disease • HypoK leads to increased ammoniagenesis which may activate the complement system • Mild Nephrogenic Diabetes Insipidus (NDI) • Defective activation of adenylate cyclase = decrease effect of vasopressin • Endocrine • Glucose intolerance = due to decreased insulin or insulin resistance
4. What is the significance of the urinary potassium levels?
Potassium Regulation • Kidney • K+ balance: Urinary K+ excretion= Dietary intake • Decreased secretion: Low K+ diet, hypoaldosteronism, acidosis, K+ sparing diuretics • GIT • dietary K+ is absorbed in the small intestine by passive diffusion • K+ is secreted in the colon through aldosterone stimulation • in diarrhea, K+ secretion by the colon is increased
Urinary Potassium level • NV = 25 - 100 meq/L • patient has decreased urinary K+ (15meq/L) • a decrease of: • <25meq/L - diarrhea • >40meq/L - diuretics
TREATMENT Therapeutic goals: to correct the K+ deficit to minimize on going losses
It is safer to correct hypokalemia via oral route in order to prevent rebound hyperkalemia if given IV • The plasma potassium concentration should be monitored frequently when assessing the response to treatment
TREATMENT Emergency Treatment of Hypokalemia A. Estimated Potassium Deficit serum K <3 mEq/L= K deficit >300 mEq serum K <2 mEq/L= K deficit >700 mEq
TREATMENT B. Indications for Urgent Replacement ECG abnormalities consistent with severe K+ depletion myocardial infarction hypoxia digitalis intoxication marked muscle weakness respiratory muscle paralysis.
TREATMENT IV infusion - for severe hypokalemia or those who cannot take oral supplementation - peripheral vein = 40 mmol/L (preferred) central vein = 60 mmol/L - rate of infusion 20 mmol/hr - mixed in NSS Continous ECG monitoring Serum potassium determination every 3-6 hours
TREATMENT Potassium chloride (KCl) -drug of choice - treat hypokalemia and metabolic alkalosis Potassium bicarbonate and citrate - more appropriate for hypokalemia associated with chronic diarrhea or RTA
TREATMENT Non-Emergency Treatment of Hypokalemia -attempts should be made to normalize K+ levels if <3.5 mEq/L. -oral supplementation is significantly safer than IV -KCL elixir, 1-3 tablespoon every day.
TREATMENT ORAL ROUTE = 200-400mmol total body K+ deficit 1 mmol/L decrease in plasma K+ concentration Plasma levels <3 mmol/L require additional 600 mmol