Restraints
Restraints. Self- Learn Packet Revised November 2002. Updated 01/07 All Staff. OBJECTIVES. At the conclusion of the self-learning packet, the learner will be able to: 1. Define the difference between Behavioral Restraints and Medical/Surgical Restraints.

Restraints
E N D
Presentation Transcript
Restraints Self- Learn Packet Revised November 2002 Updated 01/07 All Staff
OBJECTIVES At the conclusion of the self-learning packet, the learner will be able to: 1. Define the difference between Behavioral Restraints and Medical/Surgical Restraints. 2. State three benefits of limiting restraint use. 3. List at least four myths concerning the use of restraints. 4. Identify factors which increase the use of restraints. 5. State two situations in which restraints might be useful in patient care. 6. List three complications of restraint use. 7. Assess a patient for the least restrictive form of restraint. 8. Identify six alternatives to restraint use. 9. State the age-related differences in evaluation and renewal of restraints. 10. State GBMC’s philosophy for the use of restraints. 11. State GBMC’s policies for restraints use.
WHAT ARE RESTRAINTS? • Definitions • Restraints are any method, physical or mechanical device, materials or equipment attached or adjacent to the patient’s body that her or she cannot easily remove which restricts a person’s movement, physical activity, or normal access to his or her body.
Name Change • Non-Behavioral has been changed to “Medical/Surgical” This follows what JCAHO uses in their standards
PURPOSE FOR RESTRAINTS • Two types of restraints defined by JCAHO are based on the purpose for the restraints • Behavioral Restraint (Almost exclusively in ER) • Used for the control of aggressive/violent behaviororbehavior that is dangerous to self or others. • Medical/Surgical Restraint (Most common on units) • Used for care management for a patient who is exhibiting behavior that is interfering with treatment (e.g. pulling on IV, Foley, or dressings).
When Physical Restraints are NOT Considered to be Restraint Devices • When used for the purposes of security, detention or public safety on patients under forensic custody (under police guard). • When used as a voluntary mechanical support to achieve proper body position, balance, or alignment. • When used as a positioning or securing device to maintain position, limit mobility or temporarily immobilize a patient during medical, diagnostic, or surgical procedures (less than 30 minutes in children).
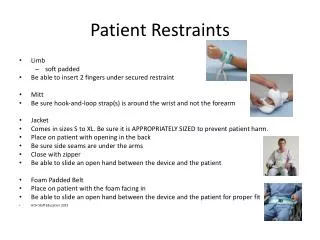
Types of Physical Restraints • Restraints may be made of soft or harder material • Neoprene (for Behavioral Restraints only) • Soft Foam Wrist or ankle straps • Roll Belts • All 4 side rails up on a bed • Mitts (secured or unsecured to bed frame) All 4 bed rails up Mitts Roll Belt Wrist/Ankle “Neoprene”
WHY LIMIT THE USE OF RESTRAINTS? Because doing so: • Benefits the patient Being able to move about freely is important for the patient’s health and a sense of dignity. • Helps the Hospital It allows the hospital to comply with laws and meet accepted care standards. • Standards and Laws limit the use of restraints 1. JCAHO 2. Federal Omnibus Budget Reconciliation Act (OBRA) of 1987 (long-term care facilities) 3. CMS (formerly HCFA) Standards (Medicare/Medicaid) 4. State Law
MYTHS ABOUT RESTRAINTS • Decreases risk of falls • Increases sense of security • Decreases lawsuits • Lowers staff costs • Improves quality of life • No other alternative
SOMETIMES RESTRAINTS CAN BE USEFUL • Allow Needed Treatment (Medical/Surgical) A combative or confused patient may have to be restrained so staff can: • Perform an exam • Treat a wound • Administer an IV • Give other needed medical treatment • Keep the Patient and Others Safe (Behavioral) • A violent patient may need to be restrained temporarily if no other calming efforts work.
RESTRAINTS CAN ALSO CAUSE SERIOUS HARM • Injuries from improperly positioned restraints • Patients get tangled in straps and choke • Patients struggle to get free and end up broken bones, cuts, concussions, or other injuries as a result • Medical complications from keeping the body and limbs in the same position for long periods can cause: • Poor circulation • Incontinence • Constipation • Weak muscles and bones • Pressure Sores • Mental and Emotional Problems Restrained patients often feel humiliated or imprisoned and become • Depressed • Agitated • Uninterested in eating, sleeping, and socializing
ASSESSING THE PATIENT IS THE FIRST STEP The health team’s goal in restraint use is to find the safest, least restrictive way to care for the patient. • Discover the Cause of the Problem • If the patient wanders, try to figure out what he or she is seeking. • If the patient is unsteady, look for underlying problems, such as poor shoes, side effects of medications, or bad eyesight. • Learn About the Patient’s Interests • A confused or agitated patient may be happier if allowed to follow familiar routines. • Give the Patient a Say • Discuss problems openly with the patient.. • If possible, ask the patient how he/she would solve the problem. • Involve Family Members • They can provide information about the patient’s habits. • They can take part in his or her daily activities. • Document a Care Plan
Alternative Interventions • Alternative means of meeting the patients needs should be attempted first. • Move patient closer to nurses station • Keep patient door open • Bed in low position • Call bell within reach • Reorient patient to environment • Conceal IV site & tubing with Stretch Netting • Decrease noise/minimize stimulation • Bed/Exit alarms with sensor pads (Posey Sitter II) • Encourage family involvement
More Alternative Interventions • Wrap Around Belt may be applied as long as it is documented patient can “demonstrate” self release with Velcro. • Exit Alarms with sensor pads for beds or chairs • Bed Alarms if available on beds.
USE RESTRAINTS AS A LAST RESORT Use Restraints only when: • You have exhausted all alternative interventions • Vital treatments depend on their use • There is a clear and present danger IF RESTRAINTS MUST BE USED • Protect the patient’s rights and dignity • Choose the least restrictive method • Document each occurrence of restraint use • Only properly trained and authorized staff may apply and remove restraints • Choose the correct restraint size - if too small, restraints may cause increased agitation and if too large, the patient can slide down in the restraint which could lead to asphyxiation.
GBMC RESTRAINT POLICIES The following policies apply to the use of restraints: • Physician orders cannot be written as “standing” or “prn”. • Restraints will not be used for the convenience of the staff. • The use of restraints will only be used to prevent the patient from harming themselves or others or when the patient is interfering with treatment.
PHYSICIAN’S ORDER CRITERIA FORBEHAVIORAL RESTRAINTS 1. Physician must be informed and a face-to-face assessment with counter signed orders within ONE hour. 2. Order must include: • Start and stop time • Date • Reason for restraint • Type of restraint used • Signature of Physician • Maximum duration 4 hours ages adults 18 and older 2 hours ages 9-17 years old 1 hour 0-8 year old 4. The physician must make a face to face re-evaluation and orders renewed every 8 hours for Adults and older every 4 hours for Children 17 and younger
PHYSICIAN’S ORDER CRITERIA FORMEDICAL/SURGICAL RESTRAINTS 1. Order must be obtained within 12 hours of initiation by the register nurse. 2. Physician must make face-to-face evaluation within 24 hours of initiation of restraints and sign order. 3. Order must include: • Start and stop time • Date • Reason for restraint • Type of restraint used • Signature of Physician • Maximum duration of order is 24 hours
Least to most restrictive • 4 Side Rails up • Roll Belt • Mittens • 1 or 2 point soft restraint • 4 point soft restraint
APPLYING RESTRAINTS • Mittens • Place hands in each mitt and secure strap ABOVE wrist bone. • Roll Belt • Position patient in the middle of the mattress. Use quick release straps to secure to bed frame. • Limb Restraint • Using a padded limb restraint, wrap the limb with the restraint and secure the plastic clip. • Tighten the restraint so that the patient is unable to pass his/her wrist through the restraint, being careful not to restrict blood flow to the extremity.
Initiation of Restraints • Only a RN may initiate the first time application of restraints. • A NST or LPN may remove and reapply restraints as needed for safety and hygiene.
Documentation • RN or Unit Secretary MUST use Order Entry in Meditech and select type of restraint ordered: Med/Surg or Behavioral. • This will generate the proper flowsheet in PCS • Med/Surg Restraint Assessment Flowsheet • Behavioral Restraint Assessment Flowsheet
Documentation • Behavioral Restraints • Q1h Assessment by RN/LPN in Meditech • Q15 mins.Observation by RN/LPN or NST on paper bedside flowsheet • Med/Surg Restraints • Q8h Assessment by RN/LPN in Meditech • Q2h Observation by RN/LPN or NST in Meditech
RESTRAINTS MONITORING BEHAVIORAL MEDICAL/SURGICAL Use Prevention Management of Aggressive Behavior (PMAB) interventions for escalating behaviors in all clinical settings. • Observe every 15 minutes for behaviors and physical conditions and document on BehavioralRestraint/Seclusion Flowsheet • Offer liquid, nutrition, comfort, and bathroom every 2 hours • Remove restraints every 2 hour for no less than 5 minutes for range of motion and skin care. • Observe every 2 hours for behaviors and physical conditions and document in Meditech • Offer liquid, nutrition, comfort, and bathroom every 2 hours • Remove restraints every 2 hours for no less than 10 minutes for range of motion and skin care.
Congratulations! • You have completed the Restraints self-learning packet. • Complete the post test.