Restraints
Restraints. What are Restraints?. Restraints are physical, chemical or environmental measures used to control the physical or behavioural activity of a person or a portion of his/her body. Laws. Policies of the Ministry of Health and Long-Term Care that are binding on long-term-care facilities


Restraints
E N D
Presentation Transcript
What are Restraints? • Restraints are physical, chemical or environmental measures used to control the physical or behavioural activity of a person or a portion of his/her body.
Laws • Policies of the Ministry of Health and Long-Term Care that are binding on long-term-care facilities • Statutes and regulations of Ontario that govern the use of restraints in facilities (the Charitable Institutions Act, the Nursing Home Act, the Homes for the Aged and Rest Homes Act) • The common law, which includes among various civil wrongs the torts of battery, assault and false imprisonment • The Criminal Code of Canada, which includes criminal offences. • The Canadian Constitution, which includes the Canadian Charter of Rights and Freedoms.
Risks of Restraints • Falls • Strangulation • Loss of Muscle tone • Pressure sores • Decreased mobility • Agitation • Reduced bone mass • Stiffness • Frustration • Loss of Dignity • Incontinence • Constipation
Risk without Restraints • Falls • Safety of self and others
Kensington Gardens Policy The Home practices a philosophy of Least Restraint.
Who? What? Why? How? When? • Least restraint means all possible alternative interventions are exhausted before deciding to use a restraint. • This requires assessment and analysis of what is causing the behaviour. All behaviour has meaning. When the reason for the behaviour is identified, interventions can be planned to resolve whatever difficulty the resident is having that contributes to the consideration of restraint use.
Kensington Gardens Policy Restraint Assessment Form must be completed prior to initial application of the restraint.
Assessment Tools • Behavioural Map • Aggressive Behaviour Risk Assessment • Cohen-Mansfield Agitation Inventory • Continence Assessment • TENA incontinence product evaluation
Environmental • Improved or altered lighting • Path cleared in resident's room/on unit • Cloth barrier across doorway • Comfortable room temperature • Privacy and dignity • Environment personalized • Wanderguard applied • Moved to secure unit • Night light
Safety • Positioning of pillows • Bed height lowered • Call bell within easy reach • Bed, Chair or Seatbelt Alarm • Side rails • Floor pad beside bed
Toileting and Continence • Individualized toileting routine • Product change • Identify bathroom using signs/symbols • Commode at bedside • Urinal at bedside
Direct Care • One to one supervision/support • Medical conditions, i.e. infections • Individualized daily routine • Move resident closer to RHA Infomation Centre • Facilitate rest periods • Limit time spent in bed
Direct Care Continued • Apply glasses and/or hearing aides • Use ambulatory aides as per Care Plan • Evaluate medical interventions i.e. catheter, feeding tube • Provide cues during care/activities
Physiological Interventions • Treatment of the underlying pathology, i.e. medication ordered • Pain management • Medication review
Psychological • Companionship • Active listening • Increase family/friends visiting • Consistent staffing • Encourage staff one to one activities • Familiarization with the environment • Behaviour management intervention • Alter sensory stimulation • Remove to a quiet area • Relaxation techniques
Life Enhancement & Programs • Teach safe transfer techniques to resident/family/responsible party • Walking and exercise programs • Incorporate exercise into daily plan of care • Meaningful individual and/or group activities • Music therapy • PT/OT consult
Nutritional Care • Provide adequate fluid/nutritional intake • Adapt provision of nutrition to resident's condition, i.e. finger food, frequent small meals, etc. • Dietitian Consult
Referrals • Attending Physician • Social Worker • Psycho-Geriatric Team • Gerontologist • External Therapeutic Assessment Program i.e. Toronto Rehab
Seating and Positioning • High back or supportive chair • Individualized seating • Chair tilt mechanism
Positioning in a Wheelchair • Hips • Level and positioned at the back of the seat • Upper Legs • Supported on the cushion to three (3) inches behind the knee • Feet • Resting on the footrests • Back • Against the back of the cushion
Positioning in a Wheelchair • Headrest • Must be on wheelchair and positioned when chair is tilted • Use of tilt • Change tilt position many times throughout the day • Padded Leg Slings • Loose to allow legs to rest back when in tilt
Things that Interfere with Good Positioning • Cushion Check- air amount, gel quality, wrong way, upside down, pommel • Medical- hip flexion restriction, back pain back kyphosis, scoliosis • Pads and transfer slings on top of cushion
Improper Positioning • Falls to the side or forward • Slides out of the wheelchair • Redness on pressure areas • Discomfort • Unable to self propel with hands or feet • Unable to engage in functional activity
Seating Cushion Materials • Foams- Pommel at the front of the cushion • Fluid Gels- Must be kneaded properly after each use • Roho Cushion- Ensure right amount of air
Roho Cushion • Correct amount: the cushion looks ¾ full • When pressure is placed on the cushion, then released, the cushion regains its shape • Too Much Air: All cells are visible, the cushion is hard, unstable and looks too large for the wheelchair
The Least Restrictive is Used Restraint Deemed Necessary
The decision to apply a restraint involves the resident and/or his family/substitute decision-maker. Documentation shows thorough assessment of the need for a restraint, including ALL alternate measures attempted Consent
Doctor’s Order • Restraint is applied on written order (or a telephone order which is cosigned) of a Physician who has attended the resident and approved the type of restraint.
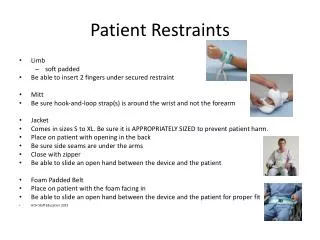
Approved Restraints • Wheelchair tray • Rear facing seatbelts • Lap restraint • Mitt restraint • Self limiting seat belt (resident cannot undo without assistance)
How Often do I check? • The resident is checked at a minimum of hourly and repositioned at a minimum of every two hours while restrained.
Documentation • Document on the Restraint Monitoring Record.
Proper Application of Seatbelts • ONLY FASTEN THE SEAT BELT IF & WHEN REQUIRED • MAKE SURE THE SEAT BELT IS IN GOOD CONDITION
Compare to a Car Seatbelt • CHECK THAT THE SEAT BELT IS TIGHTENED APPROPRIATELY • Place one flat hand between belt and resident • Too Loose is Dangerous • Position at the hips not the abdomen
NO Twisting • Ensure the belt is not twisted • Do not tie belt around arm of chair • If seatbelt is too long inform Shopper’s Home Health
Reassessment • The need for continuing use of the restraint is reassessed within 12 hours and the Restraint Monitoring record signed at the bottom by the Registered staff to indicate the continued need past twelve hours • Registered staff are also required to reassess restraint quarterly
The End!!! • Thank-you for Coming