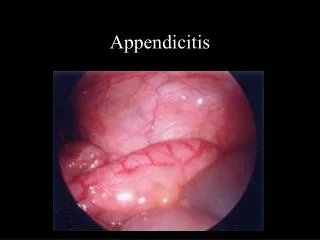
Appendicitis
Appendicitis. Standard of Care T. Topp , MDcd , FRCSC, FACS Head, Division of General Surgery. Question 1. In the USA, failure to timely diagnose acute appendicitis is the ____ most common cause for malpractice lawsuit. A. 1st B. 2nd C. 3rd D. 4th. Question 2.

Appendicitis
E N D
Presentation Transcript
Appendicitis Standard of Care T. Topp, MDcd, FRCSC, FACS Head, Division of General Surgery
Question 1 • In the USA, failure to timely diagnose acute appendicitis is the ____ most common cause for malpractice lawsuit. A. 1st B. 2nd C. 3rd D. 4th
Question 2 • The Diagnosis of Acute Uncomplicated Appendicitis mandates: A. An Emergent Operation (<8 hrs from diagnosis) B. An Urgent Operation (<24-36 hrs from diagnosis) C. No operation, as the disease can be managed medically.
Question 3 • Audience Survey: What proportion of your non-pregnant patients in whom you suspect acute appendicitis do you obtain an CT scan? A. 0-33% B. 33-66% C. 66-99% D. 100%
Question 4 • You are operating on CT proven appendicitis, but at surgery the appendix (and everything else) looks normal. Do you: A. Convert to open (or extend your open incision) and do a formal laparotomy. B. Just take out the appendix. C. Leave the appendix in, go home and blame it all on a bad virus going around. D. A & B.
So What is “Standard of Care?” • Legal: professional care and skill that might reasonably have been provided by a colleague in similar circumstances. • Appropriate measure is the level of reasonableness. • Not a standard of perfection. • The Court determines that reasonable standard through the evidence of experts.
Pre-operative Imaging Impact of computed tomography of the abdomen on clinical outcomes in patients with acute right lower quadrant pain: a meta-analysis Susan Krajewski, MD, MPH* Jacqueline Brown, MD† P. Terry Phang, MD‡ ManojRaval, MD, MSc‡ Carl J. Brown, MD, MSc‡ Can J Surg, Vol. 54, No. 1, February 2011
Cumulative pooled estimates of odds ratios of negative appendectomy rates for the computed tomography (CT) era versus the pre-CT era.
Cumulative pooled estimates of odds ratios of negative appendectomy rates for computed tomography versus clinical assessment.
Perforation Rates Numerous studies have correlated perforation with duration of symptoms and delays in presentation. similar rates of perforation between patients in the CT group and those in the clinical evaluation group (23.4% v. 16.3%, p = 0.15).
Downsides of CT Imaging Management of Acute Appendicitis: The Impact of CT Scanning on the Bottom Line Cedric V Pritchett, MD, MPH, Nick C Levinsky, BS, Yoonhee P Ha, MSc, Allard E Dembe, SCD, Steven M Steinberg, MD, FACS J Am CollSurg 2010;210:699–707 Increases cost of care Decreases contribution to margin Prolongs patient’s stay in the emergency department Delays time to operation
Time to Operation • Surgical delay correlates with appendiceal rupture • Peritonitis • Sepsis • Death • How Time Affects the Risk of Rupture in Appendicitis; Nina A Bickell, MD, MPH, Arthur H AufsesJr, MD, FACS, Mary Rojas, PhD, Carol Bodian, DrPhJ Am CollSurg 2006;202:401–406
Antibiotic Use Perioperative: reduction of SSI’s For uncomplicated (non-perforated) acute appendicitis, duration of postoperative antibiotics isunclear Post-operative antibiotic use in nonperforated appendicitis; Dinhkim Le, M.D., Wendy Rusin, A.C.N.P., Britani Hill, M.D., John Langell, M.D., Ph.D.; The American Journal of Surgery (2009) 198, 748–752
Is Surgery Really Necessary? Amoxicillin plus clavulanic acid versus appendicectomy for treatment of acute uncomplicated appendicitis: an open-label, non-inferiority, randomised controlled trial. Vons C - Lancet - 7-MAY-2011; 377(9777): 1573-9 243 pts 120 antibiotics alone, & 120 appendicectomy group 30 day post-intervention peritonitis: abx group = 8% appy group = 2% Nb. In appy group, despite CT-proven ‘uncomplicated’ appendicitis, 18% were ‘complicated’ at appendicectomy.
Is Surgery Really Necessary? • Antibiotic Group • 14/120 patients (12%) had appy in first 30 days • 30/102 (29%) had appy between 31 and 365 days • 26 of these had acute appendicitis
Normal Appendix at OR…Now What?Acute appendicitis: does removal of a normal appendix matter, what is the value of diagnostic accuracy and is surgical delay important?; SJWalkeret.al.;Ann R CollSurgEngl 1995; 77; 358-363
A case for the removal of the ‘normal’ appendix at laparoscopy for suspected acute appendicitisGrabhamet.al, Ann R Col Surg Eng 1999;81