CORONARY CIRCULATION
CORONARY CIRCULATION. Dr.Mohammed Sharique Ahmed Quadri Assistant professor Al Maarefa College. Objectives. Review the functional anatomy of coronary circulation Recognize the importance of phasic changes in coronary blood flow Describe the factors affecting the coronary blood flow

CORONARY CIRCULATION
E N D
Presentation Transcript
CORONARY CIRCULATION Dr.Mohammed Sharique Ahmed Quadri Assistant professor Al Maarefa College
Objectives • Review the functional anatomy of coronary circulation • Recognize the importance of phasic changes in coronary blood flow • Describe the factors affecting the coronary blood flow • Recognize the clinical significance (IHD)
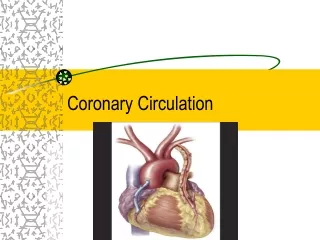
Coronary Artery & their Branches Coronary arteries arises form coronary sinus at the base of the aorta • LCA • Left Anterior Descending (LAD) • Marginal Artery • Circumflex Artery • RCA • Marginal Artery • Posterior descending Branch
Venous return • Most venous return is through 1)Ant cardiac veins & 2)coronary sinus into Right Atrium
CORONARY BLOOD FLOW • Coronary blood flow in Humans at rest is about 225-250 ml/minute, about 5% of cardiac output. • At rest, the heart extracts 60-70% of oxygen from each unit of blood delivered to heart [other tissue extract only 25% of O2.
CORONARY BLOOD FLOW Why heart is extracting 60-70% of O2? • Because heart muscle has more mitochondria, up to 40% of cell is occupied by mitochondria, which generate energy for contraction by aerobic metabolism, therefore, heart needs O2. • When more oxygen is needed e.g. exercise, O2 can be increased to heart only by increasing blood flow.
Blood flow to Heart during Systole & Diastole • During systole when heart muscle contracts it compresses the coronary arteries therefore blood flow is less to the left ventricle during systole and more during diastole. • Blood flow to the subendocardial portion of Left ventricle it occurs only during diastole
Phasic changes in coronary bld flow Effect of cardiac muscle contraction
Coronary blood flow to the right side is not much affected during systole. Reason---Pressure difference between aorta and right ventricle is greater during systole than during diastole, therefore more blood flow to right ventricle occurs during systole.
Effect of pressure gradient of aorta &diff chambers of heart • As in systole pressure in left ventricle is slightly higher than in aorta blood flow reduces • On the other hand press diff in aorta & rt ventricle & aorta & rt atrium is more during systole than diastole, coronary bld flow is not appreciably reduce during systole
As we know during systole blood flow to subendocardial surface of left ventricle is almost not there, • therefore, • this region is prone to ischemic damage and most common site of Myocardial infarction.
Effect of Tachycardia on coronary blood flow: During increased heart rate, period of diastole is shorter therefore coronary blood flow is reduced to heart during tachycardia.
Factors Affecting Blood Flow to CORONARY ARTERIES -Pressure in aorta -Chemical factors -Neural factors • NOTE—Coronary blood flow shows considerable Autoregulation.
causes of decreased blood flow to left ventricle 1-Aortic stenosis Reason---As left ventricle pressure is very high during systole, therefore, it compresses the coronary arteries more. 2-When diastolic pressure in aorta is low, coronary blood flow is decreased
Chemical factors affecting Coronary blood flow • Chemical factors causing Coronary vasodilatation (Increased coronary blood flow) • -Lack of oxygen • -Increased local concentration of Co2 • -Increased local concentration of H+ ion • -Increased local concentration of k + ion • -Increased local concentration of Lactate, Prostaglandin, Adenosine, Adenine nucleotides. • NOTE – Adenosine, which is formed from ATP during cardiac metabolic activity, causes coronary vasodilatation.
Neural factors affecting Coronary Blood Flow • -Effect of Sympathetic stimulation • -Effect of Parasympathetic stimulation • Sympathetic stimulation • Coronary arteries have • Alpha Adrenergic receptors which mediate vasoconstriction • Beta Adrenergic receptors which mediate vasodilatation
Sympathetic stimulation------Cont • Effect of sympathetic stimulation in intact body:---Epinephrine and Norepinephrine causes VASODILATATION. HOW ? • But the Direct effect of sympathetic on Coronary arteries is VASOCOSTRICTION. WHY ?
Indirect effect of sympathetic stimulation • Stimulation of sympethetic nerves release of nor adrenaline increase of H.R &force of contraction Release of vasodilator metabolites vasodilatation
Direct effect of sympathetic stimulation • When the ionotropic &chronotropic effect of noradrenergic discharge are blocked by Beta adrenergic receptor blocking drugs, injection of noradrenalin or stimulation of noradrenergic nerves in un anaesthetized animal elicits coronary vasoconstriction. • Thus direct effect of noradrenergic stimulation is V.C
Benefits of indirect effect of noradrenergic discharge • When systemic B.P decreases very low reflex increase of noradrenergic discharge Increase c.b.f sec to metabolic changes in myocardium In this way circulation of heart is preserved while flow to other organs compromised
Effect of Parasympathetic stimulation • -Vagus nerve stimulation (Parasympathetic) causes coronary vasodilatation
Special features of cardiac muscle metabolism • Heart uses primarily free fatty acids and to lesser extent glucose and lactate for metabolism. in ischemic / anaerobic conditions Derives energy from Anaerobic glycolysis Forms lactic acid (one of cause of cardiac pain )
CORONARY ARTERY HEART DISEASE • ISCHEMIC HEART DISEASE (IHD) (ANGINA PECTORIS) • MYOCARDIAL INFARCTION ANGINA PECTORIS: • THERE IS REDUCED CORONARY ARTERY BLOOD FLOW DUE TO ATHEROSCLEROSIS (CHOLESTROL DEPOSITION SUBENDOCARDIALLY -- Plaque)
RISK FACTORES OF IHD: • CIGARETTE SMOKING • HYPERTENSION • DIABETES MELLITUS • INCREASED LIPIDS ( CHOLESTROL) • OTHER FACTORS: LACK OF EXERCISE, ANXIETY etc.
IHD: • IHD IS DECREASED CORONARY BLOOD FLOW (TRANSIENT MYOCARDIAL ISCHEMIA). • PATIENT COMPLAINS OF TIGHTNESS OR PAIN IN THE MIDDLE OF CHEST (RETROSTERNAL) FOR FEW MINUTES. PAIN OFTEN RADIATES TO INNER SIDE OF LEFT ARM. • PAIN IS PRECIPETED BY EFFORT AND RELIEVED BY REST.
MYOCARDIAL INFARCTION (MI): • IT IS DUE TO OBSTRUCTION TO THE CORONARY BLOOD FLOW, ATLEAST 75 % OF LUMEN OF CORONARY ARTERY IS BLOCKED BY THROMBUS. • MI IS THE COMMON CAUSE OF DEATH.
Applied Aspect THE C A D.
Electrocardiographic changes duringexercise test. Upper trace – significant horizontal ST segment depression during exercise.
INVESTIGATIONS: • ECG • CARDIAC ENZYMES e.g. CK, LDH, TROPONIN etc. • ECHOCARDIOGRAPHY • TREADMILL EXERCISE TEST • THALLIUM STRESS TEST • CORONARY ANGIOGRAPHY • NOTE: • ECG CHANGES IN IHD: • ST DEPRESSION OCCURS IN ECG IN RESPECTIVE LEADS • ECG CHANGES IN MI: • ST ELEVATION OCCURS IN ECG IN RESPECTIVE LEADS
TREATMENT: • CORONARY DILATORS E.g. NITRATES • BETA-BLOCKERS • ANGIOPLASTY (DILATE AREA OF CONSTRICTION) • STENT • BYPASS SURGERY
Percutaneous transluminal coronary angioplasty (PTCA). (a) Coronary angiography demonstrates a severe stenosis in the proximal left anterior descending artery. (b) During PTCA a soft guidewire is passed across the stenosis and then a balloon is expanded that dilates the stenosis. (c) Post-PTC