Download
1 / 32
380 likes | 845 Vues
Coronary circulation: anatomy, blood flow and it’s regulation. Dr. Satya Pal . University College of Medical Sciences & GTB Hospital, Delhi. Important ! Why?. One – third of all deaths in the western world results from coronary artery disease.

E N D
Coronary circulation: anatomy, blood flow and it’s regulation Dr. Satya Pal University College of Medical Sciences & GTB Hospital, Delhi
Important ! Why? One – third of all deaths in the western world results from coronary artery disease. Almost all elderly people have at least some impairment of the coronary artery circulation.
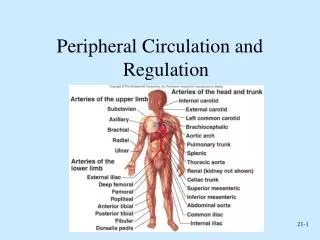
Coronary anatomy Variable 2 arteries Left coronary artery Right coronary artery Sinuses behind two of cusps of aortic valve at root of aorta Eddy currents keep valves away
Right coronary artery Originates from right aortic sinus of ascending aorta. Course: Passes anteriorly and to the right between right auricle and pulm. trunk and then descends vertically in the coronary sulcus, between right atrium and right ventricle. On reaching inf. margin of heart , turns posteriorly and continues in the sulcus onto the diaphragmatic surface and base of heart.
Branches: • Atrial branch - SA node • Right marginal branch - inf. Margin of heart. • Small branch to AV node • Posterior interventicular branch /Posterior descending artery (PDA)
LEFT CORONARY ARTERY Originates from left aortic sinus of ascending aorta. Course: Passes between pulm. Trunk and left auricle before entering the coronary sulcus.
Branches: Two terminal branches The anterior interventicular branch (left anterior descending artery) – One or two diagonal branches may arise from it. The circumflex branch - Gives off a left marginal artery.
Right coronary artery supplies • Right atrium and right ventricle • SA and AV node • Interatrial septum • Portion of left atrium • Posteroinferior 1/3 of interventricular septum • Posterior part of left ventricle
Left coronary artery supplies Most of left atrium and left ventricle, Most of interventricular septum including atrioventricular bundle and its branches.
Coronary artery dominance Approx. 60% are right-dominent, 15% are left-dominent and 25% co-dominent. If right coronary artery(RCA) supplies large portion of posterior part of left ventricle through posterior descending art (PDA) then it is called as right-dominent. If circumflex (CX), branch of left coronary artery supplies large portion of posterior part of left ventricle through PDA then it is called as left-dominent. If RCA and CX both supplies this portion of heart then it is called as co-dominant
Venous drainage Most of venous returns from heart drains through coronary sinus and ant. Cardiac veins to right atria. Coronary sinus has four tributaries: Great, middle, small, and posterior cardiac veins. Other vessels that empty directly into heart chambers includes: Thebesian veins Arteriosinusoidal vessels Arterioluminal vessels
CORONARY MICROCIRCULATION Very high density of capillaries to myofibrils, approximately 1:1; this is because of the exceptionally high metabolic demand of the heart. Uniform capillary distribution, ranges approx. 3,000 and 4,000/mm2 of tissue. Coronary capillaries are site for O2, CO2 exchange and movement of large molecules along the endothelial lining. Interestingly, capillary density is reduced in the interventricular septum and AV nodal tissue -more vulnerable to ischemia than myocardium itself.
Coronary collateral circulation Arise from different branches of the same coronary artery or from branches of two different coronary arteries. Flow through such coronary collaterals is usually negligible because the driving pressure at the two ends of the anastomoses is nearly equal. However, if the artery supplying one branch of this collateral circulation becomes severely stenotic or occluded, the large pressure reduction will divert blood flow through the patent artery and into the distribution of the occluded artery through these collateral vessels.
MECHANICS OF CORONARY BLOOD FLOW Resting coronary blood flow - 225 ml/min. About 4 to 5% of total cardiac output. At rest, the heart extracts 70-80% of O2 from each unit of delivered blood. ‘Work’ of heart under severe conditions may increase 7 to 9 folds. Coronary blood flow increases 3 to 4 folds to supply extra nutrients. The difference between maximal and resting coronary blood flow is known as coronary reserve.
Blood supply to the LV is directly dependent on the difference between the aortic pressure and LV end-diastolic pressure (coronary perfusion pressure). Blood supply to LV is inversely related to the vascular resistance to flow, which varies to the fourth power of the radius of the vessel (Poiseuille's law). Two other determinants of coronary flow are vessel length and viscosity of the blood but usually remains constant.
` Changes in aortic pressure and the impedance to flow due to physical compression of the intramural coronary arteries during the contraction-relaxation cycle governs the pulsatile pattern of coronary flow in the LV. Increased venous pressure decreases coronary blood flow as it deceases EFFECTIVE CORONARY PERFUSION PRESSURE. Blood flow in the right and left coronary arteries varies during different phases of cardiac cycle. Since aortic pressure is slightly less than LV pressure during systole and RV pressure is lower than aortic pressure.
As a result: • In LCA blood flow occurs mainly during diastole • In RCA blood flow occurs mainly in late systole and early diastole • LV subendocardium is prone to ischemic damage as blood flow occurs only during diastole. • Also blood flow is compromised when aortic diastolic pressure is reduced (e.g., severe aortic insufficiency). • When heart rate increases, diastole become short and blood flow reduced. • Not much effect to right ventricle & atria as RCA flow is continous.
In aortic stenosis – prone to develop Ischemia increased pressure in ventricle so vessels are compressed more. More O2 need due to high workload. In Congestive heart failure - Failure of pumping action Low effective coronary perfusion
Regulation of coronary blood flow Neural factors: Metabolic coronary vasodilation is partly the result of activation of the sympathetic nerves to the heart and coronary vasculature Sympathetic nerve activation produces a feed-forward β-adrenoceptor–induced vasodilation, primarily of small coronary arterioles.
There is also a feed-forward, sympathetically mediated, α-adrenoceptor–induced vasoconstriction in larger coronary arteries during exercise. This vasoconstriction occurs upstream from small coronary arterioles and serves two important functions: reduction of vascular compliance and attenuation of systolic minus diastolic flow oscillations during the cardiac cycle.
These actions assist in the preservation of blood flow to the more vulnerable LV endocardium when heart rate, contractility, and O2 consumption are elevated. Interestingly, cardiac parasympathetic nerves have a prominent role in regulating heart rate, but these have a negligible direct effect on the regulation of coronary blood flow.
Chemical factors: Nearly three fourths of coronary vasodilation during exercise is produced by yet undefined local metabolic factors that act on coronary vascular smooth muscle with or without the influence of endothelium. Many metabolic factors have been proposed to individually or collectively modulate coronary flow at the arterial or capillary level, including adenosine, nitric oxide, arterial oxygen or CO2 tension, pH, osmolarity, K+, Ca2+, and prostaglandins.
Many of these factors exert predictable direct effects. For example, hypoxia or ischemia decreases arterial oxygen tension and pH and increases CO2 tension, adenosine, K+, and Ca2+ concentrations, and serum osmolarity. Many may increase coronary blood flow, but none appear to be crucial determinants of vasodilation during exercise. For example, adenosine receptor blockade does not alter coronary blood flow under resting conditions or during exercise.
Adenosine released during hypoxia or ischemia causes coronary vasodilation and this effect is mediated by activation of KATP channels. Adenosine and KATP channels have also been implicated during reactive hyperemia after ischemia, but these mediators do not appear to be required for coronary autoregulation. Moreover, the KATP channel probably maintains a lower vascular smooth muscle tone and thus, a higher basal coronary flow during resting conditions.
References: Gray’s Anatomy for Students. 39th ed. Ganong’s Review of Medical Physiology. 23rd ed. Clinical Anesthesia. Barash. 6th ed. Wylie and Churchill-Davidson's A Practice of Anesthesia. 7th ed.