CORONARY CIRCULATION
CORONARY CIRCULATION. CORONARY CIRCULATION. The coronary circulation supplies the myocardium, a tissue that rivals the brain in terms of its nutritional demands and the critical importance of continued flow for normal function. Anatomy.

CORONARY CIRCULATION
E N D
Presentation Transcript
CORONARY CIRCULATION The coronary circulation supplies themyocardium, a tissue that rivalsthe brain in terms of its nutritional demands and the critical importance ofcontinued flow for normal function.
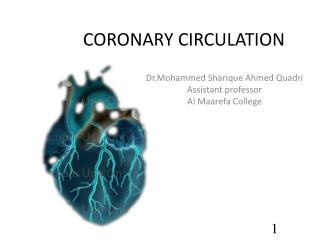
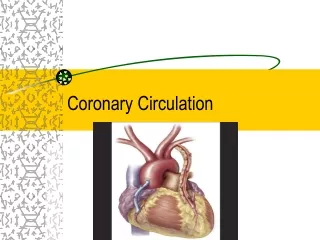
Anatomy The myocardium is supplied by left and right coronary arteries thatoriginate from the root of the ascending aorta immediately above theaortic valve. The right coronary artery generally suppliesthe right heart, whereas the left coronary artery supplies theleft. The arteries course over the heart’s surface and then dive downthrough the muscle layers. The vasculature is notable for numerouscollaterals connecting adjacent arteries and also for the presence ofprecapillary sphincters .
Coronary Circulation Only 1/10 mm of the endocardial surface can obtain nutrition from the blood inside the cardiac chamber Left coronary artery supplies mainly anterior and lateral portions of the left ventricle Right coronary artery supplies most of the right ventricle and some posterior part of the left ventricle Most coronary venous blood returns to the right atrium by coronary sinus (75% of total coronary flow) Anterior cardiac veins from right ventricle open directly into the right atrium Thebesian veins empty directly into chambers of the heart
Regulation At rest, the coronary circulation receives 5% of CO. Cardiac muscleextracts 70% of available O2 from blood, and it has a very low capacityfor anaerobic metabolism, much like the brain. This O2dependencemeans that any increase in work must be matched by an increase incoronary flow, achieved entirely through local control mechanisms.
Local controls: • Coronary resistance vessels are exceptionallysensitive to adenosine. Local control mechanisms allow for a fourfoldto fivefold increase in coronary flow when CO increases, aphenomenon called coronary reserve. • 2. Central controls: • Coronary resistance vessels are innervated byboth branches of the ANS, but their influence is overridden bylocal controls.
Coronary Circulation Right and left coronary arteries
Precapillary sphincters Precapillary sphincters comprise single smooth muscle cells wrappedaround the inlets to individual capillaries . They contractand relax with changes in local metabolite concentrations and functionas on/off switches to capillary flow.
When CO is minimal, mostsphincters are contracted (“off”), and flow is inhibited. They relax intermittently as local metabolite levels rise but again contract when theincreased flow washes the metabolites away. At rest, only a small proportion(20%) of sphincters is relaxed, and capillaries are activelyperfused, but the pattern of capillary flow shifts continually (vasomotion). When cardiac workload increases, levels of metabolic wasteproducts rise, and the sphincters spend a much greater percentageof time in the “on” position. At maximal levels of CO, all sphincters areopen all the time, and coronary flow rises to maximal levels also.
Extravascular compression Blood flow through most systemic vascular beds follows the aorticpressure curve, rising during systole and falling during diastole. Flowthrough the left coronary artery drops sharply during systole and thenrises sharply with the onset of diastole. This unique flowpattern occurs because ventricular myocytes collapse the arterialsupply vessels as they contract (extravascular compression). The effect is felt strongest during early systolebecause aortic pressure, the main force maintaining vascular patency,is at a low point. During diastole, the compressive forces areremoved, and blood surges through the musculature at peak rates.
Normal Coronary Blood Flow Resting coronary blood flow (CBF) is about 225 ml/min CBF increases in proportion to exercise or work output Phasic changes in CBF during systole and diastole
Extravascular compression in the leftventricular wall. LV= left ventricle;P= pressure.
Coronary Blood Flow Epicardial vs subendocardial CBF (intramyocardial pressure) Epicardial arteries in the outer surface supply most of the muscle Subendocardial arterial plexus is beneath the endocardium
Aort kapağı Sol koroner arter Sağ koroner arter
Control of Coronary Blood Flow Local muscle metabolism is the primary controller of CBF Oxygen demand as a major factor in local CBF regulation Normally about 70% of O2 is removed as the blood flows Role of adenosine in vasodilation And other substances
Nervous Control of Coronary Blood Flow Autonomicnervescan affectthe CBF bothdirectlyandindirectly Directstimulation of coronarybloodvessels Indirecteffectsresultfromsecondarychanges in CBF causedbyincreasedordecreasedactivity of theheart Directeffects of nervousstimuli on coronaryvasculature Parasympathetic fiber distribution is not great There is moresympatheticinnervation of coronaryvessels Constrictorreceptorsarealphaadrenoreceptors (moreepicardial) Betareceptorsarevasodilatory (more in theintramusculararteries)
Special Features of Cardiac Muscle Metabolism At rest, cardiac muscle normally consumes fatty acids to supply most of its energy instead of carbohydrates About 70% of total energy from fatty acids However, under anaerobic or ischemic conditions, glycolytic mechanism is required Glycolysis consumes tremendous amounts of blood glucose and forms large amounts of lactic acid Hypoxia, release of adenosine and dilation of coronary artery
Ischemic Heart Disease The most common cause of death Insufficient coronary blood flow Coronary ischemia, coronary occlusion and myocardial infarction – congestive heart failure Atherosclerosis as a cause of ischemic heart disease Consumption of large amounts of cholesterol and lack of mobility Development of atherosclerotic plaques in major coronary arteries
Acute Coronary Occlusion Acute coronary occlusion occurs frequently in atherosclerotic heart 1) Atherosclerotic plaque can cause a local blood clot called a thrombus Unsmooth surface, adherence of blood platelets 2) Local muscular spasm of coronary arteries may occur Spasm may result from irritation of smooth muscle Or from local nervous reflexes – plaque Spasm may lead to secondary thrombosis of the vessel
Value of Collateral Circulation in the Heart In normal heart, there is no communication between large coronary arteries But many anastomoses do exist among the smaller arteries (20-250 micrometre in diameter) This collateral circulation may delay appearance of ischemic heart symptoms
Collaterals: Collaterals are vessels thatconnect adjacent arterioles. They are usually constricted in ahealthy heart, but, if a supply vessel becomes occluded, they dilatein response to rising metabolite levels. Flow through collateralsmay prevent infarctionif the occluded vessel is small. In time,these channels enlarge to provide near-normal flow to the ischemicarea.
Flow interruption Because the ventricular myocytes extract such high levels of O2 fromthe blood, a delicate balance exists between myocardial workloadand coronary supply. If the balance is disturbed, then myocytes become ischemic and infarcted. Most commonly, this occurs due toatherosclerosisand coronary artery disease.
Atherosclerosis: Atherosclerotic lesions appear at an early agein the populations of most Western countries. They evolve to becomecomplex plaques of lipids, hypertrophied myocytes, and fibrous material. Plaques enlarge at the expense of the vascularlumen and impair blood fl ow. This causes an imbalance betweencoronary supply and myocardial demand, resulting in ischemia. Ischemic myocytes release large quantities of vasoactive compounds,such as adenosine, but vasodilators have no effect onplaque. As the O2 deficit continues, the myocytes release lacticacid, which stimulates pain fibers within the myocardium andcauses angina pectoris.
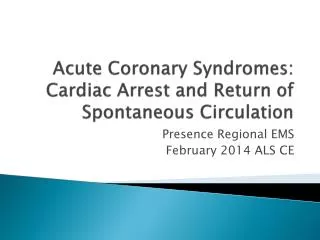
Myocardial Infarction After coronary occlusion, blood flow ceases beyond the blockage Cardiac muscle has little or no blood flow The overall process is called myocardial infarction After the onset of MI, small amounts of collateral blood begin to seep into the infarcted area Progressive dilation of local blood vessels In later stages, the vessel walls become highly permeable and leak fluid Cardiac muscle tissue becomes edematous Subendocardial infarction and systolic contraction
In the common heart attack a thrombus form in a coronary artery. Death of more than 1/3 of the left ventricle will lead to severe heart failure. Acute Myocardial Infarction Infarction
Causes of Death After Coronary Occlusion 1) Decreased cardiac output 2) Damming of blood in the pulmonary edema 3) Fibrillation of the heart 4) Rupture of the heart
Causes of Death After Coronary Occlusion 1) Decreased cardiac output (Systolic stretch and cardiac shock) Systolic stretch Incapable heart to pump sufficient blood into the peripheral arterial tree Coronary shock, cardiogenic shock, cardiac shock or low cardiac output failure Cardiac shock occurs when >40% of the LV is infarcted Death occurs in 85% of patients once they develop cardiac shock
Causes of Death After Coronary Occlusion 1) Decreased cardiac output (Systolic stretch and cardiac shock)
Causes of Death After Coronary Occlusion 2) Damming of blood in the body’s venous system Acutely reduced cardiac output leads to diminished blood flow to the kidneys The kidneys fail to excrete enough urine This adds to progressively to the total blood volume and congestive symptoms Development of pulmonary edema
Causes of Death After Coronary Occlusion 3) Fibrillation of the ventricles after myocardial infarction Sudden ventricular fibrillation Four factors into tendence for the heart to fibrillate: a) Acute loos of blood supply to the cardiac muscle and increased K ions in the extracellular space * irritability of cardiac muscle b) Ischemia of the muscle causes “injury current” * ischemic muscle cannot completely repolarize c) Powerful sympathetic reflexes develop after massive infarction – irritability increases d) Cardiac muscle weakness causes the ventricles to dilate excessively. * This increases the pathway length for impulse conduction
Causes of Death After Coronary Occlusion 4) Rupture of the infarcted area Dead heart muscle bulges outward with each contraction Systolic stretch becomes greater and the heart may rupture Loss of blood into the pericardial space and development of cardiac tamponade