PNEUMOTHORAX
PNEUMOTHORAX. ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara , Nepal. Defined as the presence of air in the pleural cavity. Negative intrapleural pressure: ~ 5mm. PNEUMOTHORAX. Spontaneous: 1. Primary spontaneous P. 2. Secondary spontaneous P.


PNEUMOTHORAX
E N D
Presentation Transcript
PNEUMOTHORAX ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara, Nepal
Defined as the presence of air in the pleural cavity Negative intrapleural pressure: ~ 5mm
PNEUMOTHORAX Spontaneous: 1. Primary spontaneous P. 2. Secondary spontaneous P. • Secondary: • Iatrogenic • traumatic
Primary spontaneous pneumothoraces • Do not have overt parenchymal disease • increased shear forces in the apex • commonly are smokers & tall young males • risk much more pronounced in female smokers • Genetic factors - Marfan’s syndrome • Defect of connective tissue
Secondary spontaneous pneumothoraces (SSP) occur in the presence of lung disease • COPD • Tuberculosis • sarcoidosis • cystic fibrosis • malignancy • idiopathic pulmonary fibrosis • Pneumocystis carinii pneumonia [PCP]) in patients with AIDS Sub pleural focus rupturing in pleural cavity
Iatrogenic pneumothorax a complication of medical or surgical procedures. results from • Therapeutic thoracentesis • Positive pressure mechanical ventilation • Pleural biopsy • Central venous catheter insertion • Transbronchial biopsy routine use of ultrasonography guided diagnostic thoracentesis is associated with lower rates of pneumothorax
Broncho pleural fistula Intra pleural pressure(0)
Symptoms: • Sudden onset (usually after a bout of coughing) of • Chest pain • dyspnoea • Asymptomatic when small Signs: • In sever cases low volume pulse with tachycardia • Collapse & signs of peripheral circulatory failure • Cyanosis (See when there is tension pneumothorax) • Vitals are normal in closed & open pneumothorax
Inspection: Dyspnoea with accessory muscles active Tracheal shift may be visible – trail’s sign Fullness of chest on affected side Diminished chest movement
Palpation: • Trachea & medistinum shifted to opposite side • Vocal fremitus – markedly diminished • Diminished expansion of affected hemithorax Percussion: • Hyper resonant note on the affected side • Liver dullness obliterated: right sided pneumothorax • Cardiac dullness shifted to opposite side
Auscultation • Vocal resonance reduced/absent • Breath sounds reduced/absent on affected side • Hamman's sign: refers to a click on auscultation in time with the heart sounds, due to movement of pleural surfaces with a left-sided pneumothorax In open pneumothorax • Amphoric breath sound due to broncho pleural fistula may be heard
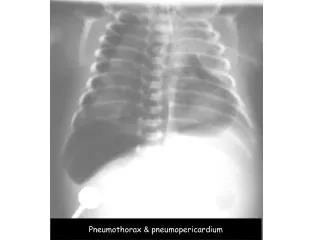
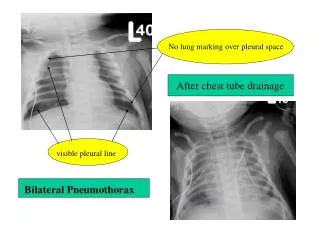
CXR -diagnostic in most cases • visible lung edge and absent lung markings peripherally • increased lucency & hemidiaphragm depression on the affected side • CXR appearance may also show features of underlying lung disease
CT chest may be required • To differentiate pneumothorax from bullous disease • Useful in diagnosing unsuspected pneumothorax following trauma • In looking for evidence of underlying lung disease
Determined by • Degree of breathlessness & lung collapse • Hypoxia • Evidence of haemodynamic compromise • Presence and severity of any underlying lung disease • Pneumothorax size
Severe breathlessness out of proportion to pneumothorax size may be a feature of tension pneumothorax • Secondary pneumothorax has a significant mortality (10%), and should be managed more aggressively. Treat also the underlying disease
Chest Aspiration Suction apparatus
Aspiration Indications Primary pneumothorax Consider aspiration if • patient breathless and/or • pneumothorax large (rim of air > 2 cm on CXR) Secondary pneumothorax Consider aspiration • patient aged > 50 years (all cases) • with small pneumothorax (rim of air < 2 cm on CXR) • minimal breathlessness
Chest drainage • Associated with significant morbidity and even mortality due to subcutaneous emphysema • not required in the majority of patients with primary spontaneous pneumothorax
Oxygen • All hospitalized patients should receive high flow (10 l/min) inspired oxygen (unless CO2 retention is a problem) • Reduces the partial pressure of nitrogen in blood, encouraging removal of air from the pleural space and speeding up resolution of the pneumothorax
Persistent air leak • Defined as continued bubbling of chest drain 48 hours after insertion In indicates: • Inability of lung to expand after the drainage • Broncho pleural fistula - communication with out side air • Will develop secondary infection and pyopneumothorax until closed by surgery
Out-patient follow-up Repeat CXR to ensure resolution of pneumothorax and normal appearance of underlying lungs Discuss risk of recurrence and emphasize smoking cessation, if appropriate
Patients should not fly for at least 6 weeks. avoid flying for a longer period, e.g. 1 year Advise about flying
Advise NEVER TO DIVE in the future, unless patient has undergone a definitive surgical procedure
Indications for cardiothoracic surgical referral • Second ipsilateral pneumothorax • Bilateral spontaneous pneumothorax • Persistent air leak (>5 -7 days of drainage) • Spontaneous haemothorax • Professions at risk (e.g. pilots, divers) after first pneumothorax
Chemical pleurodesis • As an alternative for surgery specially in case of recurrent pneumothorax • seal the visceral to the parietal pleura to prevent pleural fluid accumulating. (already described previously)
Pneumothorax acts as a one-way valve • Progressive increase in pleural pressure compresses both lungs and mediastinum • Reduced venous return to the heart, leading to hypotension and cardiac arrest • not related to pneumothorax size can occur with very small pneumothoraces in the context of air trapping in the lung from obstructive lung disease
Patients present with • Acute respiratory distress & agitation • Hypotension • Raised jugular venous pressure • Tracheal deviation away from the pneumothorax side • Reduced air entry on affected side • May present with cardiac arrest (pulseless electrical activity) • Acute deterioration in ventilated patients
Management • Give high-flow oxygen • Insert a needle into second intercostal space in midclavicular line on side of pneumothorax • Do not wait for a CXR if cardiac arrest has occurred or the diagnosis is clinically certain • Hissing air confirms diagnosis. Aspirate air until the patient is less distressed • Insert chest drain in mid axillary line afterwards