Pneumothorax and Pleural Effusions
Pneumothorax and Pleural Effusions. Update. Tension. Ann R Coll Surg Engl. 2013 Jan;95(1):61-4. doi : 10.1308/003588413X13511609956138. Thoracotomy versus VATS: is there an optimal approach to treating pneumothorax? Joshi V , Kirmani B , Zacharias J .

Pneumothorax and Pleural Effusions
E N D
Presentation Transcript
Ann R CollSurg Engl. 2013 Jan;95(1):61-4. doi: 10.1308/003588413X13511609956138. • Thoracotomy versus VATS: is there an optimal approach to treating pneumothorax? • Joshi V, Kirmani B, Zacharias J. • The 2010 British Thoracic Society guidelines recommend that a weighted decision be made by clinicians with regard to surgical intervention for pneumothorax as the video assisted thoracoscopic surgery (VATS) approach is better tolerated by patients but carries a higher rate of recurrence (5% vs 1%). • METHODS: • Overall, 163 patients underwent surgical intervention for pneumothorax at our institution and data were collected prospectively for almost 7 years. Of these, 86 patients underwent VATS under a single surgeon with extensive VATS experience to compensate for the associated learning curve while 79 patients underwent an open procedure. • RESULTS: • There was no statistically significant difference in the recurrence rate between the open and the VATS group (1% vs 3.5%, p=1.0). The VATS group was superior to the open group in terms of reduced postoperative bleeding (7.5% vs 0%, p=0.01), reduced number of intensive care unit admissions (16% vs 0%, p<0.01) and a reduced adjusted length of stay (3 vs 5.5 days, p<0.01).
Too Small? • THORACOSTOMY TUBE FLOW AND PRESSURE IN A SIMULATED PLEURAL SPACE FREE TO VIEW • Robert Evangelidis, DO*; Michael Czervinske, RRT; Timothy Dwyer, MD, FCCP; Steven Q. Simpson, MD, FCCP • Author and Funding Information • Chest. 2006;130 • PURPOSE: When patients with ARDS or interstitial lung disease develop a pneumothorax, initial insertion of a thoracostomy tube with suction to the customary 20 cmH2O often fails to reexpand the lung. Potential mechanisms for the lack of expansion include: a)lung elastance exceeds the ability of -20 cmH2O pleural pressure to give complete expansion, or b)persistent air leak exceeds the airflow capacity of the thoracostomy tube, such that -20 cmH2O is not achieved in the pleural space. We tested the ability of thoracostomy tubes of various sizes to generate intrapleural pressure changes at various levels of assumed air leak. • METHODS: We designed a chamber to simulate the volume of one hemithorax of a 70 kg human of average height. The airtight chamber allowed insertion of thoracostomy tubes of multiple sizes. Negative pressure was provided by a standard chest drainage unit attached to wall suction and regulated at -20 cmH2O. We tested tubes sized 12 Fr to 32 Fr. Airflow was adjusted in increments via an inlet valve from 0 flow to the flow at which the chest tube failed to generate any negative pressure in the chamber. • RESULTS: Results for suction at -20 cmH2O are presented in Table 1 as F15, F10, and F0, the air leaks at which intrapleural pressure rose to -15 cmH2O, -10 cmH2O, 0 cmH2O, respectively. • CONCLUSION: Small thoracostomy tubes can result in pleural pressures that are less negative than the set value when significant, but realistic air leaks are present; pneumothorax could persist due to insufficient evacuation of air from the pleural space. However, larger tubes appear to accomodate flow from even very large air leaks, suggesting that the mechanism of persistent pneumothorax in this setting may be more closely related to increased lung elastance. • CLINICAL IMPLICATIONS: Chest tubes <= 20 Fr should be avoided in the setting of increased lung elastance with pneumothorax. Further studies are needed to determine the logically appropriate approach when pneumothorax does not respond to insertion of a large tube.
Too Big? • Benson JS, Hart ST, Kadlec AO, Turk T. Small bore catheter drainage of pleural injury after percutaneous nephrolithotomy: feasibility and outcome from single large institution series. J Endourol. 2013 Sep 2. • Background and Purpose: Current literature describes placement of standard chest tubes as well as small-bore catheters for treatment of hydrothorax sustained during surgery. This study aims to better delineate the clinical utility and outcomes associated with use of small-bore catheters when compared to standard chest tubes for treating pneumothorax and hydrothorax after surgery. • Patients and Methods: Those that met inclusion criteria were divided based on the size of chest tube placed: small-bore (8-12Fr) or standard chest tube (32Fr). Analysis of clinical outcomes was performed. • Results: Out of the 735 procedures, 15 (2% of total, 7 right, 8 left) required chest tube placement for a pleural injury after PNL. Those who required chest tube placement had an average stone size of 2.1cm. Five had large bore standard chest tubes (32Fr) and 10 small bore catheters (<14 Fr) for management of pleural injury. The average length of time the chest tube stayed in place was 3.9 days (min 2, max 6) for small-bore and 4.4 days (min 2, max 7) for standard chest tubes. • There was a statistical trend toward decreased hospital stay and decreased length of time the chest tube was in place when a small bore chest tube was used. • Conclusion: The use of small bore catheters for management of hydrothorax and pneumothorax due to pleural injury have reasonable clinical outcomes when compared to standard large bore chest. • Small-bore chest tubes seem to perform better than larger tubes in treatment of spontaneous pneumothorax.
Needle Complications • Wiener RS, Wiener DC, Gould MK. Risks of Transthoracic Needle Biopsy: How High? ClinPulm Med. 2013 Jan 1;20(1):29-35 • Transthoracic needle lung biopsy is a commonly performed diagnostic procedure for pulmonary nodules and masses. To make an informed decision about whether to pursue this procedure, doctors and patients must be aware of the possible risks of the procedure. • We found the most common complication to be any pneumothorax (risk 15-25%), with pneumothorax requiring chest tube occurring less often (risk 4-6%). Hemorrhage, defined as radiographically visualized blood along the needle tract was common, but clinically significant hemorrhage was infrequent (~1%). Rare complications, including air embolism and tumor seeding of the biopsy tract, occurred in fewer than 1% of cases but were potentially serious.
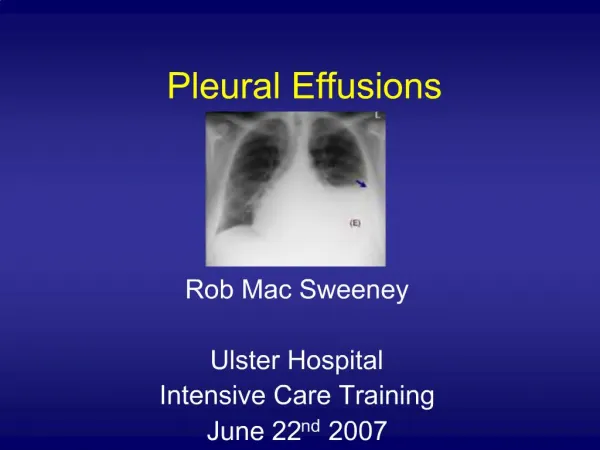
The most common causes of transudative (watery fluid) pleural effusions include: • Heart failure • Pulmonary embolism • Cirrhosis • Post open heart surgery
Exudative (protein-rich fluid) pleural effusions are most commonly caused by: • Pneumonia • Cancer • Pulmonary embolism • Kidney disease • Inflammatory disease
Other less common causes of pleural effusion include: • Tuberculosis • Autoimmune disease • Bleeding (due to chest trauma) • Chylothorax (due to trauma) • Rare chest and abdominal infections • Asbestos pleural effusion (due to exposure to asbestos) • Meig’s syndrome (due to a benign ovarian tumor) • Ovarian hyperstimulation syndrome