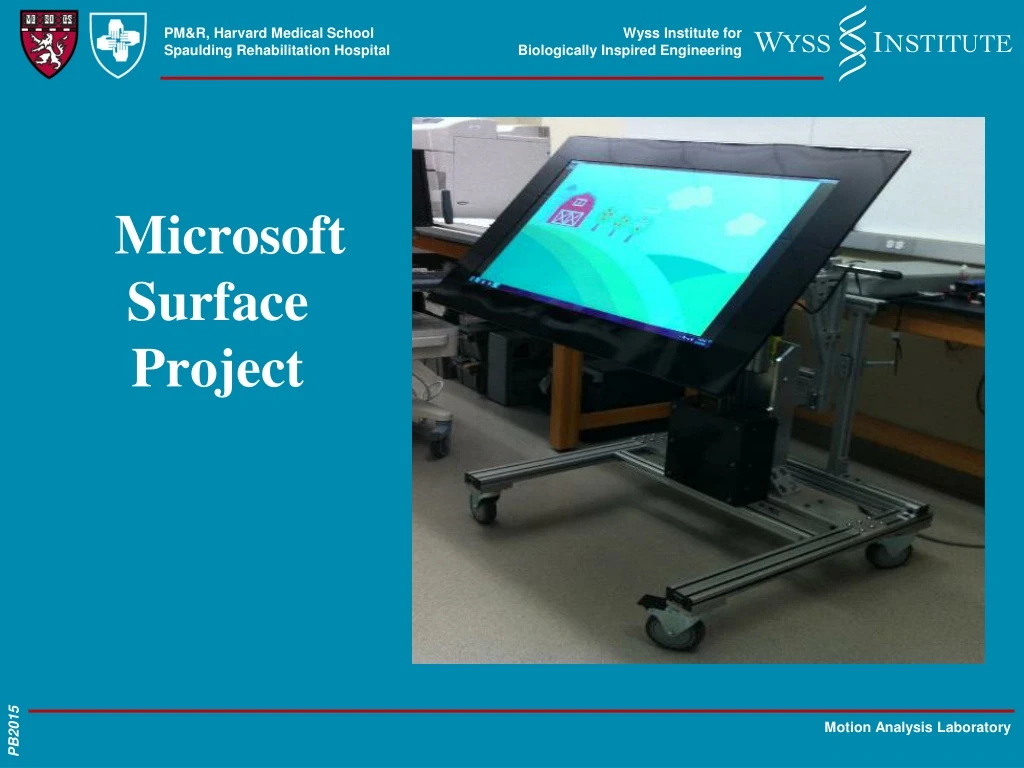
Microsoft Surface Project
Innovative therapy system for cerebral palsy utilizing Microsoft interactive touch screen technology to improve motor skills through interactive games and feedback. Study evaluates efficacy and feasibility for children aged 6-12.

Microsoft Surface Project
E N D
Presentation Transcript
I have no relevant financial disclosures. Disclosures
Cerebral Palsy • Permanent, non-progressive physical disorders • Caused by disturbances to fetal/infant brain • Affects 1 in 303 children • Causes impairments in: • movement • hearing • vision • Learning • No cure • Treatment: alleviation and maintenance of symptoms; Occupational and Physical Therapy.
Therapy services • Help minimize contractures • Improve: • range of motion • coordination • quality of movement • Provide tasks that engage and motivate • We have designed a system based on Microsoft interactive touch screen surface to address these limitations in therapy sessions.
The Platform • Five interactive games that encourage repetitive motions • Similar to iPad touch screen • Eight sensors on upper limbs • Record joint angles of shoulders and elbows • Accelerometer embedded in vest worn by the participant • Provides postural and positional data
Unique features of the tabletop • Videogames allow for repeated practice • Participants can move on their own…can lead to motor recovery • Immediate auditory and visual feedback • Progress shown in a concrete way • Pain free range of motion
Unique features of the tabletop • Children with auditory processing impairments often only learn through visual system. • Mechanics of hi/lo table allow for adaptability: • Gravity eliminated shoulder and elbow control • Easel allows for help with visual scanning, wrist • extension and holding head in neutral • Offers ability to play in sitting and standing • Adjust height for functional body mechanics • Games keep accurate record of performance • and progress.
What motor skills do the games target? • Active range of motion in gravity eliminated, against gravity and weight bearing (standing). • Fine motor skills: • Speed • Pre-writing: finger isolation • Object use: sustaining hold of adaptive tool (adaptive stylus, ball, paddle with Butterfly game)
What motor skills do the games target? • Bi-manual skills: Sub-divided into 4 categories: • Use of involved arm as stabilizer (hold paper while writing) • Ability to use involved arm symmetrically or simultaneously (pushing/pulling) • Ability to differentiate function (both arms can move to specific target) • Ability to alternate use from left to right reciprocally (playing musical instruments)
Study Design • Pilot study • Usability and feasibility of the device • Novel games: Engaging and motivating children to perform upper extremity motions
Hypothesis • Patients will be more motivated to perform therapeutic motions. • Movements to those performed in traditional therapy • Compensatory motions will be minimized by feedback from the wearable accelerometer. • Minimize failure to complete tasks. • Structure required motions that they slowly increase in difficulty and allowing interaction by patients with reduced function.
Inclusion and Exclusion criteria • Inclusion Criteria • 6-12 years old • Upper extremity dysfunction due to cerebral palsy • Able to understand, read and write in English • Able to understand and comprehend directions from occupational therapist or physician • Exclusion Criteria: • Participants may be excluded if they have severe vision impairments
Study setting • Recruitment procedures: Spaulding Rehabilitation Hospital (SRH) and Boston Children’s Hospital. • Data collection: Wyss Institute. • Data analysis: Wyss Institute and SRH. • Enroll 20 children.
Study session will last no longer than 90 minutes (including consent and assent) • Each session will be videotaped, allowing critical analysis of child's interaction with system. • Games have been divided by four motor skills: • Gross movements • Coordinated movements • Distal control • Fine motor control Study setting
Risk and benefits • We do not anticipate any physical risks to the participants from participating in this research study. • Participants enjoy using the games and received a $50 gift card.
Conclusion • Could benefit children with Cerebral Palsy by providing new treatment/rehabilitation option for those with impaired upper extremities.
Summary of Citations and Level of Evidence • A. Dunne, C. Shen, P.Bonato, Son Do-Lenh, G.O. Laighin, “Upper Extremity Rehabilitation of Children with Cerebral Palsy Using Accelerometer Feedback on a Multitouch Display”, Engineering in Medicine and Biology Society 2010 Annual International Conference of IEEE, pp 1751-1754, August 31-Sept 4, 2010 • M.Annett et al., “Using a Multi-touch Tabletop for Upper Extremity Motor Rehabilitation”, Interfaces, pp1-4, 2009 • M.Leitner, M. Tomitsch, T. Költringer, K. Kappel, and T.Grechenig, “Designing Tangible Tabletop Interfaces for Patients in Rehabilitation”, Conference and Workshop on Assistive Technologies for People with Vision and Hearing Impairments: Assistive Technology for All Ages (CVHI 2007), pp 1-7, 2007 • M. Alcañiz, V.Abarca, J.A. Lozano and N. Herrero, “Analysis of Multitouch Technology for Neurorehabilitation”, Journal of Cybertherapy & Rehabilitation, Volume 2 issue 3, Fall 2009