Immunization Guidance and Pediatric Growth Assessment in Adolescents
This document addresses immunization advice for a 14-year-old girl, including recommended vaccines and the types of vaccine-derived polioviruses (cVDPV, iVDPV, aVDPV). It also discusses abnormal EEG patterns in epilepsy, criteria for pediatric growth referrals, and proper disposal methods for biomedical waste. Additionally, it outlines the Tanner stages of development, assesses emergency management for status epilepticus in children, and highlights associated anomalies in congenital conditions. A comprehensive overview for healthcare professionals working with pediatric populations.

Immunization Guidance and Pediatric Growth Assessment in Adolescents
E N D
Presentation Transcript
Station-1 • Mother brings her 14 year old daughter for Immunization advice. She has already recd. her 10 yr Tdap and 2nd dose of MMR vaccine. • What vaccine will you advice? • Give information on two different types of vaccines ( with respect to) A: Serotype B: Schedule C: Disease protection • Define : • cVDPV • iVDPV • aVDPV
Answer-1 • HPV • Types of vaccine:
Answer-1 (2) • cVDPVs(circulating vaccine-derived polioviruses) that are associated with sustained person-to-person transmission and considered to be circulating in the environment; • iVDPVs(immunodeficiency related vaccine-derived poliovirus) isolated from immunodeficient patients who have prolonged infections after exposure to OPV; and • aVDPVs (ambiguous vaccine-derived poliovirus) isolated from a single immunocompetent AFP or paralytic poliomyelitis patient with or without additional isolates from contacts, or from healthy individuals or the environment in absence of paralytic cases.
Station-2 • Identify the abnormality in the EEG and give your diagnosis. • Mention the drug of choice and prognosis. • In case of post traumatic convulsion, what is the drug of choice and how long to continue the same.
ANSWER-2 • The 3-Hz spike and wave pattern of absence epilepsy. • Emerges from a normal electroencephalographic (EEG) background and abruptly stops with resumption of normal activity. • Valproate and Ethosuxsimide (presently unavailable) followed by lamotrigine and the benzodiazepines are the drugs of choice. • Antiepileptic drugs (AED) are required in the acute phase and can be withdrawn in a week in acute traumatic brain injury.
Station-3 • What type of growth pattern is this? • What are the criteria for referral in case of a 7 year old boy from growth monitoring program? (any 4) • In WHO BMI charts , how many centile lines are there? What is the cutoff for overweight?
Answer-3 • Familial (constitutional) growth delay • Referral criteria: ( 7 year ) • <3rd percentile or > 97th • Crossing two major percentile line( upward / downward) • Child outside Target Centile • Height <5cm/yr. Or >7 cm/yr • BMI > 85 • Girl < 8 yr with breast dev. OR Boy < 9 yr with puberty. • Eight centile line: • 5 / 10 / 25 / 50 / 75 / 85 / 90 /95
STATION-4IN WHICH COLOR BAG WOULD YOU DISPOSE EACH OF THE FOLLOWING BIOWASTE Blood agar media Used Injection needle Injection amikacin with expiry Blood soaked cotton swab Intravenous set Incinerated ash
ANSWER-4 IN WHICH COLOR BAG WOULD YOU DISPOSE EACH OF THE FOLLOWING BIOWASTE Blood agar media----YELLOW/RED Used Injection needle-BLUE/WHITE Injection amikacin with expiry-BLACK Blood soaked cotton swab-YELLOW/RED Intravenous set-BLUE/WHITE/RED Incinerated ash-BLACK TOTAL 0.5x6=3
STATION-5 WHAT ARE YOUR FINDINGS? WHAT IS YOUR PROBABLE DIAGNOSIS? What is “FLAIR” sequence in MRI study.
ANSWER-5 WHAT ARE YOUR FINDINGS? Sagittal / T1 / MRI / midline / cerebellar mass / contrast / compression of brain stem. WHAT IS YOUR PROBABLE DIAGNOSIS? Medullobalstoma What are “FLAIR”? Fluid Attenuated Inversion Recovery (FLAIR), is a pulse sequence used to null signal from fluids.
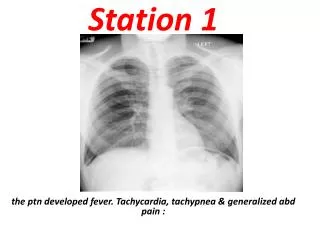
Station-6 Describe the X ray. Give your diagnosis. What associated anomalies to look for?(spinal and genitourinary)
Answer-6 Invertogram With marker Absence of gas shadow in rectum. Imperforate anus- high anomaly. GENITOURINARY Vesicoureteric reflux Renal agenesis Renal dysplasia Ureteral duplication Cryptorchidism Hypospadias Bicornuate uterus Vaginal septums VERTEBRAL Spinal dysraphism Tethered chord Presacral masses Meningocele Lipoma Dermoid Teratoma
Station-7 Please write the TANNER STAGE of the following patients: A:Girl BREAST: Breast and papilla elevated as small mound; areolar diameter increased “bud” stage. B: BOY: PUBIC HAIR:Scanty, long, slightly pigmented PENIS:Minimal change/enlargement TESTES:Enlarged scrotum, pink, texture altered Name the sub stages of adolescence with age range.
answer-7 Please write the TANNER STAGE of the following patients: A:Girl : SMR- 2 BREAST: Breast and papilla elevated as small mound; areolar diameter increased “bud” stage. PUBIC HAIR:Sparse, lightly pigmented, straight, medial border of labia B: BOY: SMR-2 PUBIC HAIR:Scanty, long, slightly pigmented PENIS:Minimal change/enlargement TESTES:Enlarged scrotum, pink, texture altered Name the sub stages of adolescence with age range. Early(10-13) / mid(14-16) / late (17-20)
Sattion-8 5 year old brought in status epilepticus to emergency room.. Write the steps in management including the drug / dose / precaution. As per “IAP expert committee guideline-2009”
Answer-8(1) Ref: Indian Pediatrics August 2009 Establish ABCs: Establish IV access, draw blood for laboratory investigations IV glucose, calcium, or pyridoxine (in neonates and infants) ↓ IV Lorazepam 0.1 mg/kg OR IV diazepam 0.2 mg/kg followed by IV phenytoin/fosphenytoin (If no IV access use PR diazepam 0.5 mg/kg or buccal/nasal/IM midazolam 0.2 mg/kg; intraosseous access could be considered as a next step if IV still not available.) ↓ Repeat Lorazepam/ Diazepam once more SOS (5-10mins) ↓ IV fosphenytoin 20 PE (phenytoin equivalent)/kg/phenytoin 20 mg/kg(30 mins) (Consider transfer to PICU facilities as child at risk of refractory status) ↓
Answer-8(2) IV valproate (1:1 diluted NS 20-40 mg /kg over 1-5 minutes; given as continuous infusion at a rate of 5mg/kg/hr, if required. OR IV phenobarbital 15-20 mg/kg (Re-assess airway again; consider tracheal intubation, if the airway is compromised or the patient develops respiratory depression)(45-60 min) ↓ Transfer to a PICU set-up is mandatory as the child has refractory SE and will need intensive monitoring in a tertiary PICU set up. ↓ Midazolam infusion (loading dose of 0.2 mg/kg, followed by 0.1 mg/kg/h titrate every 15 mins upwards by 0.05 mg/kg/h till control; maximum dose 2 mg/kg/h) OR Propofol infusion/ Pentothal infusion (Propofol should not be routinely recommended in view of significant morbidity and mortality in children) ↓ General anesthesia if above steps fail (Tertiary hospital set-up essential) In refractory status epilepticus needing coma producing therapies (Pentothal etc) EEG monitoring preferably continuous should be used, if available. It should also be used if coma persists despite control of convulsive status epilepticus (to exclude non convulsive status epilepticus)
Station-9 A 2 year old boy with bad eczema was investigated for recurrent infections of his ear and chest. The following results were obtained: • Hb 14 g/dl • WBC 10000 • Platelet count 20000 • IgA twice normal • IgG twice normal • IgM half normal • Isohaemogglutinins ABSENT • Ques: what is the most likely diagnosis? • Ques: what is the mode of Inheritance? • Ques: What information can you derive from CBC / ESR (w.r.t. Primary Immunodeficiency.
Answer-9 • Wiskott-Aldrich syndrome • X-linked Recessive • COMPLETE BLOOD COUNT, MANUAL DIFFERENTIAL, AND ERYTHROCYTE SEDIMENTATION RATE • Absolute lymphocyte count (normal result rules against T-cell defect) • Absolute neutrophil count (normal result rules against congenital or acquired neutropenia and • [usually] both forms of leukocyte adhesion deficiency, in which elevated counts are present even between infections) • Platelet count (normal result excludes Wiskott-Aldrich syndrome) • Howell-Jolly bodies (absence rules against asplenia) • Erythrocyte sedimentation rate (normal result indicates chronic bacterial or fungal infection unlikely)
Station-10 • At what age would you expect a child to copy the above shapes correctly? • Name the pervasive developmental disorders.
Answer-10 P.D.D. • Autism 4 ½ 3 yr 4 • Asperger syndrome • Rett syndrome • Childhood integrative disorder • PDD- otherwise not specified
Station-11 • Case of dengue fever are being increasing reported in your city. A 6 year old boy presents to you with fever, body ache, and pain abdomen for 6 days. There is a history of bleeding from nose for last 1 day. The child is restless, pulses are feeble, has a petechial rash over limbs, and tender hepatomegaly. The systolic BP is 50 mm of Hg. Platelet count is 27000 /cu.mm. • Write your complete diagnosis ( as per WHO Classification) • Write down the initial fluid management.( wt 20 kg) • Does this child require platelet transfusion? • Name other(ANY 4) diseases to be notified.
Answer-11 • DHF III / DSS • IV 400 ml rapid bolus over 30 min. of RL / DNS / NS / ½ NS ( ANY ONE IS CORRECT) • YES
STATION-12 • A 2 day old neonate, 1400 gram , given surfactant at birth, and is on the ventilator for RDS. • PIP 27 • PEEP 5 • RATE 35/min • FiO2 0.4 • T-Insp. 0.4sec. • ABG: pH 7.57 / PaCO2 : 22/ PaO2 156 / HCO3 19 • Give complete diagnosis. • Name one change in ventilator setting to normalize the ABG. • Name 3 long term complications that can occur in this neonate due to the blood gas abnormalities.
Answer-12 • Uncompensated resp. alkalosis with hypoxia. • Reduce PIP • Answer-3 • ROP • Bronchopul. Dysplasia • Periventricular leukomalacia
Station-13 An infant presents with failure to thrive, chronic airway infections, fatty stools, and elevated sweat chloride levels. Which of the following pedigrees best illustrates the inheritance pattern of this disease? Likely diagnosis? Name each inheritance pattern..
Answer-13 • Pattern B : autosomal Recessive • Cystic Fibrosis • Patterns • A: mitochondrial • B: Auto.Rec. • C: X-linked Rec. • D: Auto. Domin. • E: X-linked Domin ( allow Auto. Domin as well)
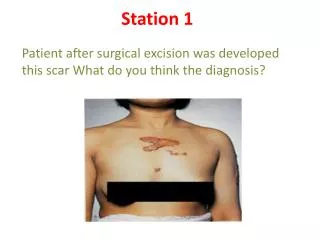
Station-14 A B C These are three skin manifestations of the same disease. Identify them. Give diagnosis. Write other skin manifestations seen in this condition.
Amswer-14 • Images : • Adenoma sebaceum • Shagreen patch • Ungualfibroma (Konen’s tumors) • Tuberous sclerosis. • Other skin manifestations: • Ash leaf macule • Café au lait spot • Skin tags • Flat plaques on forehead • Tuft of white hair on scalp / eye lids
Station-15 • Ques A : • A 15 year old boy presented to casualty with a small wound while clearing manure in the stable. His last dose of tetanus immunization was 11 years ago. • What anti–tetanus ( if any) treatment would you prescribe? • Ques-B: • A 10 year old girl has been bitten on her left palm. She is rushed immediately brought to Casualty. • Mention the steps in management. Including dose / site /schedule of the treatment.
Answer-15 • Ans. A: • Inj. tetanus toxoid and • Anti tetanus immunoglobulin. • Ans.B: • Clean the wound with water and antiseptic. • Do not cover the wound. • Inj rabies vaccine 0.5 ml ( verorab) or 1 ml (rabipur)I.M. on Day 0 , 3 , 7 , 14 , 28 (or 30). • Anti rabies human immunoglobulin ( 20iu /kg) if not available anti rabies equine immunoglobulin(40 iu/kg)….. As much as possible should be infiltrated locally .(At least Half the doses hould be given locally and other half IM on the deltoid of the same limb). • Rabies vaccine and immunoglobulin to be given on two DIFFERENT sites.
Station-16 • Define the following • Incidence • IMR-infant mortality rate • Give formula for each of them: • Mean • Median • Standard deviation • P value • Specificity • Positive predictive value
Answer-16 • Incidence: The number of NEW cases occurring in defined population during a specified period of time. • Mean • Median • Standard deviation • P value • Specificity • Positive predictive value
Station-17 As per Revised National Tuberculosis Control Program • Achievement of at least________ % cure rate through supervised short course chemotherapy. • Augmentation of case finding activities through quality sputum microscopy to detect at least_______ % of estimated cases. Malaria Program • In NMEP the program was divided into 4 phases (name them) • Modified plan of operation under NMEP came into force from______ year. • Endemic areas under modified plan of operation under NMEP is defined as annual parasite index ( API) > ________.
Answer-17 • 85 % • 70 % • Malaria program (NMEP) phases: • a) Preparatory • b) Attack • c) Consolidation • d) Maintenance • 1977 • E. 2
Station-18 6 year old presented with pain in throat with difficulty in respiration 1 day. Throat examination showed palatal weakness with white patch on tonsil Name two common complications in this situation? What is the name of stain IN THE SLIDE? Write differential diagnosis of white patch on tonsil.
Answer-18 • Diphtheria • Compliactions: • Myocarditis • Neuroparalysis • Both leading to Hypoxia • Upper Airway obstruction • Albert Stain • Differential Diag.: • Strep. Throat • Exudative tonsillitis • Infectious Mononucleosis
Station-19 Describe the ECG. Give diagnosis. Give causes (any 4) Name two congenital long QT interval syndromes.
Answer-19 • The PR interval is 0.24 seconds (240 ms) in this patient and all P waves conduct to the ventricle with constant but prolonged PR interval. • First-degree atrioventricular block. • Calcium channel blockers, beta-blockers, digoxin, and amiodaron • Acute myocarditis • Infective endocarditis, diphtheria, rheumatic fever, Chagas disease, Lyme disease • Collagen vascular disease • Athletic training • Cogenital long QT interval: • Romano-Ward syndrome (RWS) • Jervell and Lange-Nielsen syndrome (JLNS)
Station-20 2 yr old boy brought with H/o intermittent painless rectal bleeding for last few months. The stool is described as brick colored or currant jelly colored. There is anemia. Following study was performed. Name the isotope. Identify the dark areas on the film. What is the diagnosis? How to enhance the yield of this test?
Answer-20 • technetium-99m (pertechnetate) • Stomach • Ectopic acid secreting mucosa in meckel’s diverticulum • Urinary bladder • Meckel diverticulum • The uptake can be enhanced with various agents, including ranitidine, glucagon, and gastrin.
Station : 21Counsel the mother, whose child has being diagnosed with Haemophilia A
Answer : 21Counsel the mother, whose child has being diagnosed with Haemophilia A
Observed Station : 23 37 weeks, Primi with PIH with IUGR, Amniotic fluid clear, DID NOT cry or Breathe, Limp.
Observed Station :24 Administer HIB Vaccine to this 4 month old child who is otherwise normal.
Answer-24 Administer HIB Vaccine to this 4 month old child who is otherwise normal.