Download
1 / 17
170 likes | 267 Vues
Investigating patient well-being during radiotherapy treatment for breast cancer patients post-operation. Focus on utility, inconvenience, and decision-making under different scenarios. The study provides theoretical contributions related to aggregating utilities and decision utility versus experienced utility. The feasibility of measuring patient well-being using a proposed method is discussed.

E N D
Unstable Preferences: A Shift in Valuation or an Effect of the Elicitation Procedure?* Peter P. Wakker; joint with S.J.T. Jansen, A.M. Stiggelbout, M.A. Nooij, E.M. Noordijk, & J. Kievit (2000), Medical Decision Making 20, 62–71.Dept. of Economics, Univ. of Amsterdam *Grant from the Dutch Cancer Society We examin the well-being (utility/quality of life) of patients during radio-therapy treatment.
2 Clients: a class of patients with breast cancer. I skip medical details. post-operative early-stage breast-cancer patients who had completed primary treatment (lumpectomy or mastectomy). Decision problem: p cure no radiotherapy no cure 1-p p+ cure, inconvenience • drawback: • Unpleasant. • Side effects. • Different for different classes of patients radiotherapy no cure, inconvenience, palliation Advantage: (1) palliation (2) better cure-chance 1-p-
3 Radiotherapy scenario (“inconvenience”) Meeste overslaan "I skip the medical details" • Practical: Daily hospital visit for radiotherapy over a period of six weeks; • Physical: skin reactions (warm, red breast and dry skin), general fatigue; • Psychological:feelings of anxiety, worry about one's future health; • Social: limitations to work or other daily activities, restrictions on leisure activities.
The evaluations of the outcomes 4 Decision analysis approach: Probabilities delivered by epidemiologists. Topic of this lecture: How get utilities? We focus on one aspect:Utility ("well-being") during radio-therapy. So, what I called "inconvenience" in the decision tree. Even we focus more, see later. Anyway, this is the context within which our study took place.
5 Project led to two theoretical contributions(in 3 papers): Will be mentioned later. • Aggregating utilities (over time): A method for measuring utility if strong intertemporal interactions and no time separability; • Decision utility versus experienced utility: a design for detecting the causes of differences.
n U(x1,…,xn) = j=1wjuj(xj,x) 6 "That is, on what may come after. Anticipated utility." It depends crucially. Problem: U(radio-thpy) depends on prognosis. No time separability; no usual “QALYs.” We face special case of aggregating utility You cannot measure it out of its context, as if a chronic health state, as do all conventional measurement methods in health economics. Direct doorklikken wat xj en u(xj) is. (xj health state during period j) with uj(xj) depending on other xis. "its parameters" Model too general to measure/identify. No separability/utility-independence. Multivalent and hypercube models (Farquhar & Fishburn 1981, OR) are too general. Too much interactions
½ (b1,c2,…,cn) (b1,d2,…,dn) ½ g1 g1 7 We developed “anchor levels.” to measure utility g1b1 are anchor levels if ½ (b1,c2,…,cn) ~ (b1,d2,…,dn) ½ multivariate risk aversion NIET opbrengen
8 Identify and measure u1(x1,x): • U(x) U(g1x) and g1x ~ (p,x; 1p,b1x):u1(x1,x) = 1/p 1; • U(g1x) U(x) U(b1x) and x ~ (p,g1x; 1p,b1x): 0 u1(x1,x) = p 1; • U(b1x) U(x) and b1x ~ (p,g1x; 1p,x): u1(x1,x) = -p/(1-p) 0. Say that looks difficult but actually is easier for subjects, because within context.
9 Theorem. {bi,gi}, i=1,…,n, are anchor levels if and only if U(x1,...,xn) =wjuj(xj,x)+W(x) whereijwjuj(xj,x)+W(x) is independent of xj, i.e. U depends on xi only through wjuj(xj,x), and everything identifiable ... Is theoretical foundation. In: Wakker, Jansen, & Stiggelbout (2002), "Measuring Attribute Utilities when Attributes Interact." Axiomatization not just l'art pour l'art. Shows how to measure well-being of patients during radiotherapy, and shows that these numbers are meaningful inputs in other analyses.
10 Feasibility: • Jansen, Stiggelbout, Wakker, Vliet Vlieland, Leer, Nooy, & Kievit (1998), “... Utilities for Cancer Treatments: Feasibility of a Chained Procedure ...," Medical Decision Making 18, 391–399. • Feasibility enhanced because • health states can be taken in natural context; • need not be taken as chronic. Remember, preceding analysis was not to have fancy maths, but to be able to measure well-heing of patients during radio-therapy.
11 We used the method in the second paper, the one awarded. So, we can measure U(radio-therapy). NIET decision versus experienced opbrengen, want we gaan al focussen op een vraag. We focus on one question, often debated in the medical field: I'm going to a new slide for it.
12 Whose utilities are “better” (using Kahneman’s terminology): -decision: of patients prior to treatment? or -experienced: of patients during treatment? They face the decision! They know better! By some strict interpretations of the economic paradigm, these things are not even defined, being based on introspection. A dilemma!
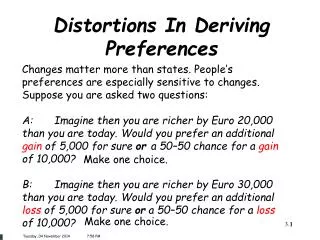
13 Example: prior to blindness: U(blind) = 0.7. On a scale with U(†) = 0, U(perfect health) = 1. After gotten blind: U(blind) = 0.9. decision time incon- sisten- cy! experienced Question to patient: "why different?" Answer: No lack of info; changed tastes! Dilemma:Use 0.7 or 0.9 in cost/effectiveness studies and policy decisions?
p cure no radiotherapy no cure 1-p p+ cure, inconvenience radiotherapy no cure, inconvenience, palliation 1-p- 14 Or, imagine that prior well-being of radiotherapy = 0.7. posterior well-being of radiotherapy = 0.9. How decide in decision problem of p. 2:
15 Wouldn’t matter if utilities were to coincide. So, how about that? Common finding in health domain: measurements of decision U < measurements of experienced U. Common conclusion:decisionU<experienced U. Then the dilemma persists! If you allow me to be repetitive. If measurements give this inequality, then so will the real values?
16 We: Conclusion of last < is premature! Problems in measurement! For example, prior descriptions of predicted outcomes may be systematically too negative: Doctors may emphasize downsides of impaired health states. Then decision utility itself need not be lower. Question: How test such a hypothesis? Announce receipe (see notes)
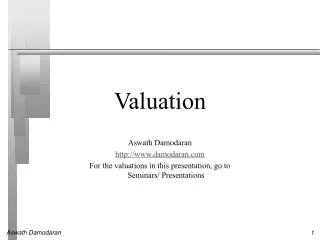
:control scen. (ch.tpy; dec.uty) 1 .9 .8 U .7 .6 .5 .4 bef.r.tpy bef.r.tpy bef.r.tpy bef.r.tpy bef.r.tpy during r.tpy during r.tpy during r.tpy during r.tpy during r.tpy during r.tpy before r.tpy Adapta-tion? Relate to usability in C/E analyses. 17 :actual state (expnd uty) :radio tpy. scen. (dec. uty) IMAGINE that same before and after r.th. (Dit voordat "Yes" in derde kolom geklikt wordt.) Remind them that here actual, circle, r.th. Red:sign (.05) Green:not sign nonusable in C/E nonusable in C/E nonusable in C/E usable in C/E (4) When scale omes up, repeat that: death-perfect-health before sho-wing 2nd x, announce it. (1) Valuati-on shiftagain. after adap., discuss before clicking on Adapta-tion? Our data:non-cor-respond-ing des-cription. Common-ly found discrep-ancy; adapta-tion? (the com-mon inter-pretation.) Not adap-tation! Non-cor-respon-ding des-cription. (2) “well I’m reaching the boundary of my imagination, anyway, if valuation shifts are found, it is trouble and you can’t just use the measured utilities. Have to correct or so. We applied this scheme in our application, and here is what we found. Application-specific! Yes! No. Valu-ationshift. (3) Before 3d column, first: “of course the measurement of r.th.scenario during treatment can be different. Let us now consider the case that it is bigger, say same as circle. (2) "As said before, there can be other explanations, and we show how to test for those." (5)