Download
1 / 27
280 likes | 840 Vues
Intravenous Fluids in Children NPSA Guidelines. Dr Pam Cupples SPAN Meeting Friday the 20 th of April 2007 Dunkeld. Aims. Historical approach to fluid management based on Holliday & Segar’s ‘4/2/1’ formula Problems with hypotonic fluids in the Paediatric Population NPSA guidelines.

E N D
Intravenous Fluids in Children NPSA Guidelines Dr Pam Cupples SPAN Meeting Friday the 20th of April 2007 Dunkeld
Aims • Historical approach to fluid management based on Holliday & Segar’s ‘4/2/1’ formula • Problems with hypotonic fluids in the Paediatric Population • NPSA guidelines
Maintenance Fluid Requirements Maintenance fluid requirements parallel energy metabolism • Energy Expenditure - using tables and nomogram Darrow et Pratt, JAMA 1950 • Body surface Area – Crawford et al, Pediatrics 1950 • Age - Wallace, Am. J. Clin. Path. 1953 • Weight – Holliday & Segar, Pediatrics 1957
‘healthy’ infants and children Energy expenditure at rest and during activity Energy expenditure equated to water requirements 1ml of water required to burn 1 calorie 1.2mls water are consumed 0.2mls water are produced 3mmols/kg of Na 2mmol/kg of K Infants require ~ 100cal/kg/day Older Children ~ 75cal/kg/day Adults ~ 35cal/kg/day Calorie Requirements 100cal/kg/day <10kg 50cal/kg/day 10-20kg 20cal/kg/day >20kg Holliday & Segar’s Formula Hypotonic fluid 0.18% NaCl with 4% Dextrose
How we got the ‘4-2-1’ rule Calorie Requirements Based on Weight 0-10kg: 100cal/kg/day 10-20kg: 1000cal + 50cal/kg/day for each kg over 10kg > 20kg: 1500cal + 20cal/kg/day for each kg over 20kg Water Requirements – ‘ 4-2-1 rule’ 0-10kg: 100 water/kg/day ( 4ml / kg/ hour) 10-20kg: 1000 water + 50 water/kg/day for each kg over 10kg ( 2ml/kg/hour) > 20kg: 1500 water + 20 water/kg/day for each kg over 20kg (1ml/kg/hour)
Holliday & Segar - the flawsThe Maintenance Need for Water in Parenteral Fluid Therapy– Pediatrics 1957 WEIGHT • Illner et al 2000 - resting energy expenditure is based on fat free mass • Accounts for 80% of the BMR but only 7% of the total body mass • Calculating energy expenditure based on weight significantly over estimates the calorie requirements and hence the water requirements
Energy Expenditure • No allowance for the different energy expenditure in acute disease / post surgery • Actual energy expenditure is 50% lower than values used by Holliday & Segar • Briassoulis et al, 2000 • Lindahl et al, 1988 • Lower energy requirements due to : • 50% of calorie expenditure allowed for growth • Catabolic state • Inactivity • PICU setting – IPPV / sedated and paralysed • Exceptions – fever,sepsis & burns
Water Losses • Insensible water losses 27ml/kg/day • Heeley & Talbot , 1955 • 50% of this value –Lamke, 1977 • Skin 7ml/kg/day • Lungs 5ml/kg/day • Urinary losses • 50-60ml/kg/day Holliday & Segar, 1957 • No allowance for non-osmotic stimuli for ADH • Stress, pain, surgery, fever • Drugs – opioids, NSAIDs • Urinary volume reduced to 25ml/kg/day • Endogenous water production from tissue catabolism • in acute illness
Hazards of Hypotonic FluidsAcute Hospital Acquired Hyponatraemia • Prescription of hypotonic fluids • Provision of excess free water in conditions where patient unable to excrete the excess water load • Non – osmotic stimuli for ADH
Stress Pain Post-operative period Sepsis Pyrexia Nausea & vomiting Co-existing medical conditions CNS infections Respiratory disorders Metabolic & endocrine disorders Drugs Morphine NSAID’s SSRI’s Barbiturates Carbamazepine Clofibrate Isoprenaline Chlorpropamide Vincrisitine Non Osmotic Stimuli for ADH Secretion
Hazards of Hypotonic FluidsAcute Hospital Acquired Hyponatraemia • Acute Hyponatraemia • Na < 136mmols/L occurring within 48 hours • Severe hyponatraemia if Na < 130mmols/L • Or any level of hyponatraemia associated with clinical signs • Risk group • Children • Premenopausal women • Hypoxia • Hyponatraemic encephalopathy • 50% of children with Na<125mmol/L • 8% mortality rate • Risk of developing hyponatraemia with hypotonic fluids is 17.2 times than with isotonic fluids • Choong et al, 2006 • Children have a poorer outcome than adults for a given level of hyponatraemia
Acute Hospital Acquired Hyponatraemia – children at risk Common symptoms • Headache • Nausea & vomiting • Weakness Advanced signs • Seizures • Respiratory arrest • Dilated pupils • Decorticate posturing • Coma • Pulmonary oedema
Risks of Hypotonic Fluids 50 cited cases of child death or neurological injury in the international literature 4 deaths and 1 ‘near miss’ in the UK since 2000 • Post-op setting in previously healthy children • Minor surgical procedures
Conclusions • Hypotonic fluids are not benign but potentially dangerous • 17.2 times more likely to develop hyponatraemia with hypotonic fluids than with isotonic • Isotonic fluids offer a safe alternative to hypotonic fluids with no risk of hypernatraemia • Fluid regimes should be tailored to the individual • Appropriate monitoring • Weight, baseline U&E’s
Background to the NPSA • March 2003 – RCA asked by the RCPCh to issue warning re. The use of 0.18% Saline in 4% Dextrose • November 2004 – Inquiry set to investigate the deaths of 3 children from hyponatraemia following a documentary • Audit in 2004/2005 – few anaesthetists had seen the warning • NPSA – advice to healthcare professionals on how to reduce risk develop solutions and introduce them into clinical practice
NPSA Plan of Action • July 2005 – form an internal working group to assess problem • August 2005 – External working group appointed after • October to November 2005 – meetings of the external group to discuss evidence collected • Dec 2005 – draft of the safe practice recommendations • Jan-Feb 2006 – Wide stakeholder consultation on draft • April 2006 – publish NPSA guidance
NPSA – Patient safety alert 22: Reducing the risk of hyponatraemia when administering intravenous infusions to children (Alert 5 of 5)Applies to all paediatric patients from 1 month to 16 years28th March 2007 • Remove 0.18% NaCl / 4%Dextrose from general stock • Produce and disseminate clinical guidelines for the fluid management of paediatric patients • Adequate training and supervision of staff • Reinforce safe practice • Promote the recording and reporting of hospital acquired hyponatraemia • Audit programme to ensure that the NPSA recommendations are being adhered to
NPSA guidelines • Template for developing local guidelines for the prescription & monitoring infusions in children • Importance of rigorous clinical and laboratory monitoring • Prescription of fluids same importance and consideration as other medicines • Fluids must be individualised • Calculate fluid balance and monitor plasma Na
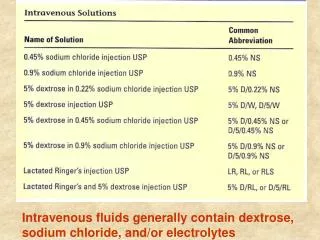
Oral fluids preferable to iv Resuscitation Fluids – bolus of 0.9% saline Deficit – calculated and replaced as 0.9% saline or 0.9% saline with 5% dextrose Replace over 24 hours Maintenance – do not use 0.18% saline with 4% dextrose 0.45%saline with 5% dextrose Children at high risk – only isotonic fluids Peri and post operative Na levels lower end of normal or <135mmol/L Volume depleted Hypotension CNS infection Head injury Bronchiolitis Sepsis Excessive gastric / GI losses Chronic conditions – CF,IDDM Salt wasting syndromes
Ongoing losses Assessed 4 hourly Replacement fluid should reflect the type of electrolyte composition of the fluid being lost Isotonic safest choice Monitoring Robust regime Weight of child Baseline and daily measurements of Na, K, urea & Cr More frequent if Na already low or clinical picture changes Training E-modules to assess current level of competencies & knowledge Doctors in training (80-90%) Review their fluid prescriptions IV Prescription Charts Review & redesign – include guidelines on fluid presciptions Monitoring data required How to calculate fluid requirements NPSA Guidelines
Arieff et al, BMJ 1992 Prospective clinical case study 16 children who died or developed permanent neurological damage 0.34% incidence of post-op hyponatraemia (83 affected out of 24,412 patients) 8.4% mortality rate (7 deaths) Halberthal et al, BMJ 2001 23 patients 13 hyponatraemic in post-op period 15 referred to critical care 11 from wards and 4 from other institutes Seizures (18) and vomiting (17) 5 had Rx withdrawn due to brainstem herniation 1 patient sustained permanent, severe neurological damage 16 / 23 receiving maintenance fluids at 50% more than recommended values
Paut et al, Ann Fr Anesth Reanim 2000 7 Children 3-6 years ASA 1-2 Scheduled surgical procedures Vomiting, seizures, status or GCS (5/7) 1 respiratory arrest with Na 120mmol/L All had hypotonic fluids 3/7 IPPV Rx – fluid restriction, NaCl 1 death McRae et al, Int J Pediatr Otorhinolaryngol 1994 3 post-op tonsillectomy patients 2 deaths
Choong et al, 2006 • Systematic review • 6 studies satisified inclusion criteria • 2 unmasked RCT • 1 non randomised CT • 3 observational studies • Mean Na in hypotonic group –3.39mmol/L • Small number of studies with small group size • Total of 404 patients
Holliday & Segar 0-10kg: 100cal/kg/day 10-20kg: 1000cal + 50cal/kg/day for each kg over 10kg > 20kg: 1500cal + 20cal/kg/day for each kg over 20kg