Download
1 / 136
1.37k likes | 1.72k Vues
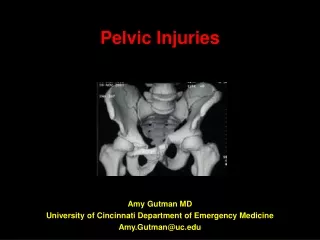
Radiographic Evaluation, Anatomy, and Classification of Pelvic Ring Injuries. Kyle F. Dickson, MD Chief of Orthopaedics, Charity Hospital Director of Orthopaedic Trauma Tulane University Created March 2004 Reviewed April 2007. Palpable Bony Landmarks. Symphysis Pubis

E N D
Radiographic Evaluation, Anatomy, and Classification of Pelvic Ring Injuries Kyle F. Dickson, MD Chief of Orthopaedics, Charity Hospital Director of Orthopaedic Trauma Tulane UniversityCreated March 2004Reviewed April 2007
Palpable Bony Landmarks • Symphysis Pubis • Anterior Superior Iliac Spine (ASIS) • Iliac Wing • Posterior Superior Iliac Spine (PSIS)
Pelvic Ring • 2 innominate bones • 1 Sacrum • Gap in symphysis < 5 mm • SI joint 2-4 mm
Important Stabilizing Ligaments • Posterior Iliosacral • Anterior Iliosacral • Sacrospinous • Sacrotuberous • Symphyseal
Important Muscles • Gluteus Maximus • Iliopsoas • Rectus Abdominus
Possible Arterial Bleeders in Pelvic Injuries • Iliolumbar artery • Superior gluteal artery • Lateral sacral artery • Internal iliac artery • Internal pudendal (active bleeding most commonly found)
Neurologic Damage • L5 & S1, most common • L2 to S4 possible • Dependent on location of fracture and amount of displacement
Denis, CORR 1988 • Sacral Fractures – Neurologic Injury • Lateral to foramen – 6% injury • Through foramen – 28% injury • Medial to foramen – 57% injury
Pohlemann, CORR 1994 • Amount of displacement move important then location
Potentially Damaged Visceral Anatomy • Blunt vs. impaled by bony spike • Bladder/urethra • Rectum • Vagina
Pelvic Ring • No inherent stability • Ligaments give the pelvis stability
Symphyseal Ligaments • Resist external rotation in double-leg stance • Rami act as struts to resist compressive and internal rotation in single leg stance • Sectioning causes little pelvic instability
Ghanayem, J Trauma 1995 • Abdominal wall contributes to pelvic stability (laparotomy increased pelvic displacement in cadaveric model)
Sacrum • Inlet View Reverse keystone where compression forces displace sacrum anteriorly • Outlet View True keystone compression locks sacrum into pelvic ring • Small rotating movements during gait
Posterior Ligaments • Ant. SI Joint – resist external rotation • Post. SI and Interosseous – posterior stability by tension band (strongest in body) • Iliolumbar ligaments augments posterior complex
Sacrotuberous (sacrum behind sacro-spinous into ischial tuberosily vertically) Resists shear and flexion of SI joint Sacrospinous – (anterior sacral body to ischial spine horizontally) resists external rotation
Normal SI Joint Motion with Gait • < 6 mm of translation • < 6° rotation • Intact cadaver resist 5,837 N (1,212 lbs)
Nachemson, Acta Orthop Scand 1966 • Sitting 710 N (160 lbs) at each Si joint • Lying 196 N (44 lbs) • Lateral decubitus 686 N (154 lbs) • Standing 980 N (220 lbs)
Sitting or Double Leg Stance • Pubic rami tension and compression posteriorly • External rotation injury – displaces in sitting or double leg stance
Single Leg Stance • Tension shear posteriorly and compression of rami • Will displace internal rotation injury
Direction of Force • Anteroposterior • Lateral compression • Vertical shear
Stability – ability of pelvic ring to withstand physiologic forces without abnormal deformation
Translational Deformities • X axis – Diastasis or impaction • Y axis – Caudad or cephalad displacement • Z axis – Anterior or posterior displacement
Rotational Deformities • X axis – Flexion or extension • Y axis – Internal rotation or external rotation • Z axis – Abduction or adduction
Deformity of Pelvis • Defined from an anatomically positioned pelvis in space • Deformity a combination of rotational & translational deformities
Deformity of Pelvis (cont.) • Does not deform around a single point but can be represented as a vector from a normally positioned pelvis • Acute deformity difficult to measure but direction often able to be determined
Pelvic Instability • These injuries which will have worsening deformity • Physical exam and radiographic evaluation
Determining Stability • Integrity of posterior bone and ligament, unstable = vertical plane displacement • Some partial instability in rotation
Physical Exam • Symmetrical palpable ASIS, iliac wing, and symphysis • ASIS compression test • Iliac wing compression test
Radiographic Evaluation • Anteroposterior view (AP) • Inlet view (40° caudad) • Outlet view (40 ° cephalad) • CT