Download
1 / 1
10 likes | 240 Vues
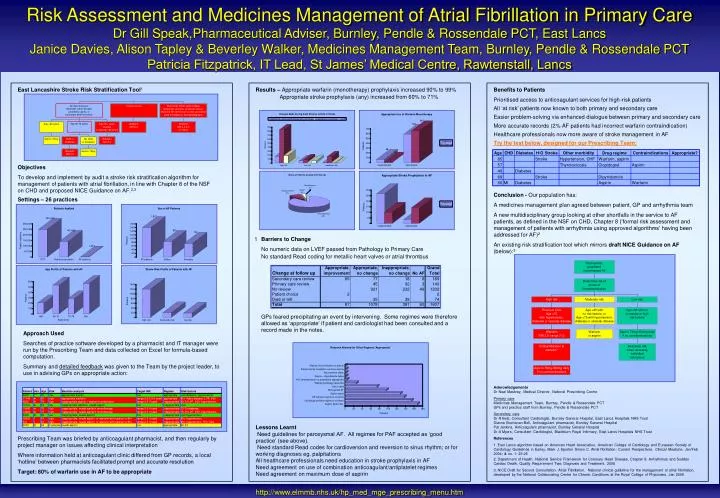
Dr Gill Speak,Pharmaceutical Adviser, Burnley, Pendle & Rossendale PCT, East Lancs Janice Davies, Alison Tapley & Beverley Walker, Medicines Management Team, Burnley, Pendle & Rossendale PCT Patricia Fitzpatrick, IT Lead, St James’ Medical Centre, Rawtenstall, Lancs.

E N D
Dr Gill Speak,Pharmaceutical Adviser, Burnley, Pendle & Rossendale PCT, East Lancs Janice Davies, Alison Tapley & Beverley Walker, Medicines Management Team, Burnley, Pendle & Rossendale PCT Patricia Fitzpatrick, IT Lead, St James’ Medical Centre, Rawtenstall, Lancs Risk Assessment and Medicines Management of Atrial Fibrillation in Primary Care East Lancashire Stroke Risk Stratification Tool1 Results – Appropriate warfarin (monotherapy) prophylaxis increased 90% to 99% Appropriate stroke prophylaxis (any) increased from 60% to 71% Benefits to Patients Prioritised access to anticoagulant services for high-risk patients All ‘at risk’ patients now known to both primary and secondary care Easier problem-solving via enhanced dialogue between primary and secondary care More accurate records (2% AF patients had incorrect warfarin contraindication) Healthcare professionals now more aware of stroke management in AF Try the test below, designed for our Prescribing Team: Objectives To develop and implement by audit a stroke risk stratification algorithm for management of patients with atrial fibrillation, in line with Chapter 8 of the NSF on CHD and proposed NICE Guidance on AF.2,3 Settings – 26 practices Conclusion - Our population has: A medicines management plan agreed between patient, GP and arrhythmia team A new multidisciplinary group looking at other shortfalls in the service to AF patients, as defined in the NSF on CHD, Chapter 8 (‘formal risk assessment and management of patients with arrhythmia using approved algorithms’ having been addressed for AF)2 An existing risk stratification tool which mirrors draft NICE Guidance on AF (below):3 1 Barriers to Change No numeric data on LVEF passed from Pathology to Primary Care No standard Read coding for metallic heart valves or atrial thrombus GPs feared precipitating an event by intervening. Some regimes were therefore allowed as ‘appropriate’ if patient and cardiologist had been consulted and a record made in the notes. Approach Used Searches of practice software developed by a pharmacist and IT manager were run by the Prescribing Team and data collected on Excel for formula-based computation. Summary and detailed feedback was given to the Team by the project leader, to use in advising GPs on appropriate action: Acknowledgements Dr Neal Maskrey, Medical Director, National Prescribing Centre Primary care Medicines Management Team, Burnley, Pendle & Rossendale PCT GPs and practice staff from Burnley, Pendle & Rossendale PCT Secondary care Dr R Best, Consultant Cardiologist, Burnley General Hospital, East Lancs Hospitals NHS Trust Dianne Buchanan-Bell, Anticoagulant pharmacist, Burnley General Hospital Pat Jenkins, Anticoagulant pharmacist, Burnley General Hospital Dr A Myers, Consultant Cardiologist, Blackburn Royal Infirmary, East Lancs Hospitals NHS Trust References 1. East Lancs algorithm based on American Heart Association, American College of Cardiology and European Society of Cardiology Guidelines in Earley, Mark J, Sporton Simon C. Atrial fibrillation: Current Perspectives. Clinical Medicine. Jan/Feb 2004; 4: no. 1: 22-26 2. Department of Health. National Service Framework for Coronary Heart Disease, Chapter 8. Arrhythmias and Sudden Cardiac Death. Quality Requirement Two: Diagnosis and Treatment. 2005 3. NICE Draft for Second Consultation. Atrial Fibrillation. National clinical guideline for the management of atrial fibrillation, developed by the National Collaborating Centre for Chronic Conditions at the Royal College of Physicians. Jan 2006 Lessons Learnt Need guidelines for paroxysmal AF. All regimes for PAF accepted as ‘good practice’ (see above). Need standard Read codes for cardioversion and reversion to sinus rhythm; or for working diagnoses eg. palpitations All healthcare professionals need education in stroke prophylaxis in AF Need agreement on use of combination anticoagulant/antiplatelet regimes Need agreement on maximum dose of aspirin Prescribing Team was briefed by anticoagulant pharmacist, and then regularly by project manager on issues affecting clinical interpretation Where information held at anticoagulant clinic differed from GP records, a local ‘hotline’ between pharmacists facilitated prompt and accurate resolution Target: 80% of warfarin use in AF to be appropriate http://www.elmmb.nhs.uk/hp_med_mge_prescribing_menu.htm