ATRIAL FIBRILLATION
180 likes | 488 Vues
ATRIAL FIBRILLATION. NILOFAR RAHMAN, MD AMIT KUMAR, MD. DEFINITION A SVT with uncoordinated atrial activation with constant deterioration of atrial mechanical function

ATRIAL FIBRILLATION
E N D
Presentation Transcript
ATRIAL FIBRILLATION NILOFAR RAHMAN, MD AMIT KUMAR, MD
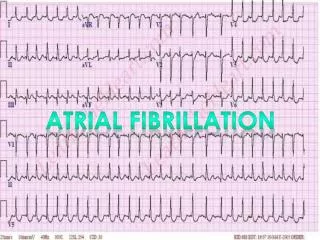
DEFINITION • A SVT with uncoordinated atrial activation with constant deterioration of atrial mechanical function • On EKGs it is defined by replacement of consistent P waves with rapid oscillations that vary in size, shape and timing ass. With an irregular RVR when AV conduction is intact.
CLASSIFICATION • PAROXYSMAL:Self terminates< 7 days, usu, within 24 hrs. • PERSISTENT: > 7 days, terminate spontaneously or by cardioversion • PERMANENT: > 1 YR, CV attempted or failed • LONE: Without any structural heart disease
ASSOCIATED DISEASES • HTN: 1.4 fold increase risk • CHD: when complicated by acute MI or heart failure • CASS trial: RR was 1.98 in 7 yrs • VALVULAR HEART DISEASE: • MS, MR, TR: 70% RISK • MS, MR: 52% • ISOLATED MS: 29% • HYPERTROPHIC CMP: • CONGENITAL HEART DISEASE • OTHERS: hyperthyroidism, PE, COPD, lupus myocarditis • OSA: reduced reccurence with treatment
CLINICAL MANIFESTATIONS • SYMPTOMATIC OR ASX EVEN IN SAME PT. • PALPITATION/CP/DYSPNEA/FATIGUE/LIGHTHEADEDNESS/SYNCOPE • EMBOLIC COMPLIC. OR HEART FAILURE • POLYURIA: ANP • ASS. RVR- CMP
EVALUATION • H&P: • EKG: verify AF • CXR: lungs, vasculature and cardiac outline • ECHO • TTE: size and function of chambers, valvular heart diseases • TEE: thrombi in left atrium • TSH • ADDITIONAL TESTING: • EXERCISE TEST • HOLTER/EVENT MONITOR
RATE VS. RHYTHM CONTROL • AFFIRM AND RACE TRIALS: 2 CONCLUSIONS- • Embolic event occur in equal frequency • lower incidence of primary end point with rate control strategy
TREATMENT • RATE CONTROL • Beta blockers • Calcium channel blockers • Digoxin • GOALS: HR<80 bpm, 24 hr. Holter average <100 bpm, HR < 110 bpm in 6 min. walk • Non pharmacologic method: radiofrequency ablation and pacemaker implantation
RHYTHM CONTROL • PHARMACOLOGIC • DIRECT CURRENT CARDIOVERSION • Anticoagulation for 3-4 weeks before CV • Anticoag for 1 month after CV • usu done in hemodynamically unstable pts. • success rate is 75-93%, inversely related to atrial size and duration
…contd. RHYTHM CONTROL • Maintenance of NSR: • 20-30% maintain NSR > 1 yr. w/o antiarrythmics • duration of <1 yr, atrial size < 4 cm. • reversible causes • Amiodaroneis known to be most effective • CTAF and AFFIRM trials • Flecainide and propefenone in those without heart disease
ANTICOAGULATION IN AF • RISK OF STROKE IS 3-5% WITHOUT ANTICOAGULATION • CHADS2 SCORE • SCORE OF 0: ASA • SCORE 1-2: ASA/WARFARIN • SCORE > 2: WARFARIN, INR GOAL 2-3
DABIGATRAN • APPROVED IN 10/10 • RE-LY TRIAL EVALUATED SAFETY OF 2 DOSES • RESULTS: • Rate of stroke was lesser • High dose - more effective than warfarin • Risk of bleeding was lesser in low dose • All-cause mortality was reduced
DISADVANTAGES • Twice dosing • High cost • Lack of an antidote • Dose adjustment for those with CKD • lack of long term safety data