Cellulitis
Cellulitis. Darren Wilson Antibiotic Pharmacist Royal Bournemouth Hospital. Some Facts. Definition – “a diffuse spreading inflammation of the subcutaneous tissue caused by bacterial infection” True incidence not really known Not reportable so no definitive data

Cellulitis
E N D
Presentation Transcript
Cellulitis Darren Wilson Antibiotic Pharmacist Royal Bournemouth Hospital
Some Facts • Definition – “a diffuse spreading inflammation of the subcutaneous tissue caused by bacterial infection” • True incidence not really known • Not reportable so no definitive data • SSTI’s account for around 176 admissions per 100,000 of the UK population • Accounted for ~3% of emergency medical consultations in one UK hospital • A 2006 study in the USA found an incidence of 24.6 cases per 1000 person years
Bites / Stings Skin breaks E.g. fissures, cuts, puncture wounds, lacerations Other infections E.g.Athletes foot Diabetes PVD Ischaemic ulcers Obesity Lymphoedema Risk Factors
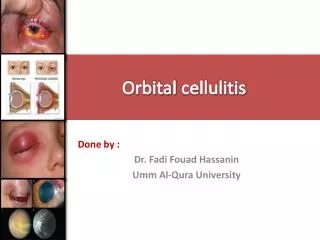
Clinical Signs and Symptoms • Tenderness and heat • Pain • Erythema • Swelling
Clinical Signs and Symptoms • Tenderness and heat • Pain • Erythema • Swelling • Malaise • Fever / Chills • Poorly demarcated borders • Local abcesses
Complications • Abcess formation • Septicaemia • Lymphoedema • Necrotizing skin infections
Causes • Microbiological diagnosis is rare • Primarily Gram +ve organisms • Group A Streptococcus (also groups B,C and G) • Staphylococcus aureus • Less commonly: • Gram –ve’s such as E.coli, Pseudomonas • Anaerobes - esp secondary to wounds, ulcers, diabetic foot • Some rare other causes
Treatment • Prompt Antibiotics • Severe cases need hospital admission for IV therapy • Non-severe cases can be managed at home with oral antibiotics • Bed rest and elevation of the affected part • Analgesia • Good skin care
Which patients should be admitted to hospital? • Signs of septicaemia (hypotension, tachycardia, severe pyrexia, confusion, tachypnoea or vomiting) • Continuing or deteriorating systemic signs after 48 hours of treatment • Unresolving or deteriorating local signs despite trials of first and second line antibiotics
Antibiotic Therapy • MUST choose a drug which covers Group A Streptococcus and Staph aureus* • Flucloxacillin is the first line choice (good activity against both organisms) • Amoxicillin is highly active against Group A Strep but not against Staph. aureus • Several alternatives in penicillin allergy including Macrolides (erythromycin, clarithromycin), Clindamycin, Cephalosporins (Cefuroxime) and some others *Group A Strep is the most common in Lymphoedema
Antibiotic Therapy (2) • Very occasionally use two agents in combination most usually Benzylpenicillin + Flucloxacillin • In severe case may add another agent such as Gentamicin to give good gram –ve cover • If MRSA is suspected will need an anti-MRSA agent such as Vancomycin or Teicoplanin
Outcomes • Cellulitis usually responds fully to appropriate antibiotics • IV Abx can be switched to PO once a good response occurs • Total course lengths of 7-14 days are usually required • In lymphoedema longer courses may be necessary – the BLS recommend a minimum of 14 days from the time a definite clinical response is observed
Other Considerations • Cellulitis is often recurrent especially in lymphoedema • “in case” antibiotics are recommended for any patient who has had a previous attack • 2 weeks of amoxicillin, flucloxacillin or clindamycin • Prophylactic antibiotics - the jury is undecided! • BLS suggest this should be offered to patients who have two or more attacks per year • Penicillin or erythromycin is appropriate • Initially for 1 – 2 years (lifelong if further episode) • Limited evidence only – a 2014 meta analysis of 5 trials (535 pts) concluded that prophylaxis is effective but much more research is needed