PERIORBITAL CELLULITIS
PERIORBITAL CELLULITIS. Periorbital Cellulitis versus Orbital Cellulitis. Definition. I nfection of the eyelid and surrounding skin anterior to the orbital septum.

PERIORBITAL CELLULITIS
E N D
Presentation Transcript
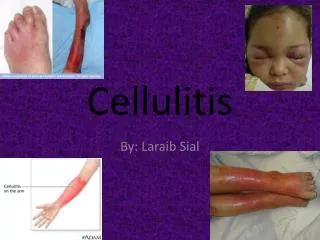
Definition • Infectionof the eyelid and surrounding skin anterior to the orbital septum. • Periorbitalinfection causes erythema, induration, and tenderness of the periorbital tissues, with patients rarely showing signs of systemic illness. • Violaceousdiscoloration of the lid is more commonly associated with Haemophilusinfluenzaebut may be associated with infection with Streptococcus pneumoniae.
Causes • Staphylococcus aureus • Streptococcus pyogenes • Because Streptococcus pneumoniaeis the most common cause of bacteremia in young children, it is also the most common cause of periorbitalcellulitis • Haemophilusinfluenzae type b is becoming a rare cause because of the prevalence of H. influenzae vaccinations.
Risk Factors • Insect bites and stings, animal bite, or human bite • Injury or trauma with a break in the skin (skin wounds) • History of peripheral vascular disease • Diabetes-related or ischemic ulcers • Recent cardiovascular, pulmonary (lung), dental or other procedures • Use of immunosuppressive or corticosteroid medications
Risk Factors • Rheumatoid arthritis patients have a higher risk of infection compared to the general population due to a number of factors: • - Concomitant medication use -- for example, taking a DMARD (methotrexate) and a coricosteroid(prednisone) • - Disease activity • - The more severe the disease, the higher the risk of infection
DIFFERENTIAL DIAGNOSIS OF OTHER CAUSES OF PERIORBITAL CELLULITIS
Prolonged Drug Use • The patient was maintained on PREDNISONEand HYDROXYCHLOROQUINE SULFATE BID for 14 years
Prednisone • Maintenance Drug: • Low dose oral glucocorticoids retard the development and progression of bone erosion • It is a useful additive therapy to control the symptoms. • It may also have a long term protective effect against bone damage. • When combined with DMARDs, it can be beneficial in controlling signs and symptoms and afford long term retardation of bone erosion
Prednisone • Side Effects: OCULAR EFFECTS • Exophthalmoses • Posterior sub-capsular cataracts • Retinopathy • Ocular hypertension • Glaucoma • Optic neuritis • Temporary or permanent visual impairment • Secondary fungal and viral infections of the eye
Prednisone • Side Effects: MUSCULOSKELETAL EFFECTS • Myopathy(myalgia, muscle wasting, muscle weakness) • Impaired wound healing • Bone matrix atrophy (osteoporosis) • Bone fractures such as vertebral compression fractures or fractures of long bones • Avascularnecrosis of femoral or humoral heads • Glucocorticoid-induced osteoporosis
Hydroxychloroquine Sulfate • Maintenance Drug: • DMARDs retard the development of bone erosion. • It has been noted that rheumatoid factor, C-reactive protein and the ESR all decline upon usage of the drug. • This is started as soon as diagnosis of RA is established. • This also modifies inflammatory component of RA, and hence its destructive capacity. • Hydroxychloroquineis usually used when other DMARDs fail therapy.
Hydroxychloroquine Sulfate • Side Effects: OCULAR EFFECTS • Ciliarybody: disturbance of accommodation with symptoms of blurred vision. This is dose-related. • Cornea: transient edema, punctate to lineal opacities, decreased corneal sensitivity. Corneal changes are fairly common, but reversible • Retina: Macula: edema, atrophy, abnormal pigmentation (mild pigment stippling to a “bull’s eye” appearance), loss of foveal reflex, elevated retinal threshold to red light in macular, paramacular, and peripheral retinal areas
Prednisone • Side Effects: NEUROMUSCULAR EFFECTS • Skeletal muscle palsies or skeletal muscle myopathy or neuromyopathy leading to progressive weakness and atrophy of proximal muscle groups which may be associated with mild sensory changes, depression of tendon reflexes and abnormal nerve conduction