Download

1 / 13
140 likes | 564 Vues
Periorbital vs Orbital Cellulitis. Morning Report 7/25/12 Melanie McIntosh. Anatomy. Pathogenesis. Rhinosinusitis ( especially ethmoiditis ) Extension of external ocular infection Stye , dacryocystitis / dacryoadenitis Skin trauma (insect bites, acne, surgery) Dental abscess

E N D
Periorbitalvs Orbital Cellulitis Morning Report 7/25/12 Melanie McIntosh
Pathogenesis • Rhinosinusitis (especiallyethmoiditis) • Extension of external ocular infection • Stye, dacryocystitis/dacryoadenitis • Skin trauma (insect bites, acne, surgery) • Dental abscess • Hematogenous seeding
Epidemiology Periorbital Cellulitis Orbital Cellulitis • More common overall • Age <5yrs • M=F • All ages • Average: 6.8 yrs • 2:1 M>F • Associated with sinusitis and URIs • More common in winter
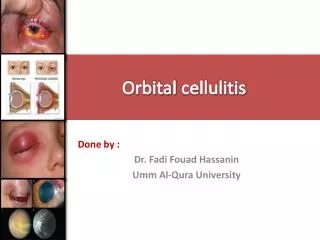
Clinical Presentation • Unilateral erythema, edema, warmth, tenderness of eyelid • Fever, systemic illness can be seen • Orbital Cellulitis – increased intra-orbital pressure • Vision changes (i.e. diplopia) • Ophthalmoplegia • Proptosis • Chemosis • Limited EOM • Reduced visual acuity • Abnormal light reflexes
Differential Diagnosis • Edema • Allergic Reaction • Hypoproteinemia • Sickle Cell – orbital wall infarction, subperiosteal hematoma • Proptosis • Orbital Pseudotumor • Graves Disease - exophthalmos
Diagnostic Work-up • Periorbital Cellulitis – typically clinical dx • EOMI • Orbital Cellulitis • Elevated WBC, CRP, ESR (but DO NOT use alone to make the diagnosis!) • Wound Culture • CT Scan c contrast • Edema unable to examine eye • CNS involvement • Loss of visual acuity, proptosis, ophthalmoplegia • Worsening/no improvement after 24-48hrs tx
Contrast CT – Orbital Cellulitis • Proptosis • Intraorbital free air • Diffuse fat infiltration
Indications for Inpatient Admission • Diplopia, loss of visual acuity, abnormal light reflexes, proptosis, ophthalmoplegia • CNS Involvement • Lethargy, vomiting, HA, seizures, focal deficits, altered mental status • Inability to fully examine eye
Pathogens • 75% Staph & Strep • S. epidermidis, S. aureus, S. pyogenes • MRSA • H. influenza type b • S. pneumo • Polymicrobial • Especially seeding from dental abscess
Treatment Periorbital Cellulitis Orbital Cellulitis • Staph and Strep coverage • MRSA • PO = IV • 7-10 days • Should see improvement in 24-48hrs • Coverage for Staph, Strep, and organisms causing rhinosinusitis • MRSA • 10-14 days • Start with IV, but may switch to PO after seeing improvement • Surgery
Complications – Periorbital Cellulitis • Recurrent Periorbital Cellulitis (RPOC) • 3 infections within 1 yr, spaced by at least one month • Not due to treatment failure • Underlying causes • Atopy • Nonbacterial organisms – HSV, Mycobacteria • Collagen Vascular Disorders • Structural abnormalities • Immunosuppression
Complications – Orbital Cellulitis • Cavernous Sinus Thrombosis • Acute or slowly progressive symptoms of orbital cellulitis • Proptosis, periorbital edema, and ophthalmoplegia • Late Signs: vision loss, meningismus • Intracranial Infections • Subdural empyema, Intracerebral abscess, Extradural abscess, Meningitis • Optic Nerve Damage – vision loss • Septic emboli • Compression ischemia