Download
1 / 23
230 likes | 424 Vues
Registries in Primary Care: Using Data to Support Innovative Health Care Delivery. Heather Brislen, MD. Associate Professor of Medicine, University of New Mexico School of Medicine. Center for Health Systems & Informatics Research New Mexico VA Health Care System.

E N D
Registries in Primary Care: Using Data to Support Innovative Health Care Delivery Heather Brislen, MD Associate Professor of Medicine, University of New Mexico School of Medicine Center for Health Systems & Informatics Research New Mexico VA Health Care System
Center for Health Systems and Informatics Research • Based at New Mexico VA Health Care System • Supported by 2-year grant from VISN 18 • Staff • Core informatics faculty • Technical staff • Service representatives • Pharmacy • Nursing Service • Medicine Service • Ambulatory Care Service
The Old Paradigm • The “acute care” model • Symptom-driven • Disease well-established • Opportunity for prevention is lost • Contact initiated by patient • Often unaware of his/her own health status • Not knowledgeable about the disease
The Old Paradigm • Medical care is delivered on a case-by-case basis • Cannot determine which conditions are the most problematic or where the process has failed • Cannot assess demand for services or allocate resources • Cannot prioritize patients based upon likelihood of benefit • Cannot identify and disseminate “best practices”
The Old Paradigm • Visit-based care • Most difficult to coordinate • Most expensive option • Most vulnerable to access barriers (geographic, economic, and social) • Misses people who do not attend clinic (often the most needy) • Treatment tied to the availability of appointments – not response to the intervention • Long delay between when findings are “discoverable” and discovered • The “one-size fits all” appointment never fits anybody • Too soon for some problems and too late for others • Too short for some patients and too long for others
The Old Paradigm • Physician-centric • Creates “bottleneck” in workflow • Physician often assigned menial tasks while team members are under-utilized. • Team disabled in physician’s absence
PCMH • The Patient-Centered Medical Home • PROMISES: • Team based care, population management, complicated case management, improved access via better utilization of team members (top of your license work) • SHORTCOMINGS: • Often remains physician-centered and physician-dependent • Top of your license work requires coaching and support that may or may not be available when needed • There is still no fail-safe mechanism to prevent “falling through the cracks”
Health Informatics • Widespread adoption of electronic health records • Very rapid implementation driven by financial incentives • Data collection over entire health care systems • PCMH-ready setting, primed for a team approach
VA Electronic Medical Records • Fully implemented in 1996 • Archives going back 15 years • Largest health system in US • Corporate Data Warehouse • 25 million patients • 52 billion records • Near real-time data acquisition • Considered the principal reason VA has outperformed private sector in processes, outcomes, and costs for years
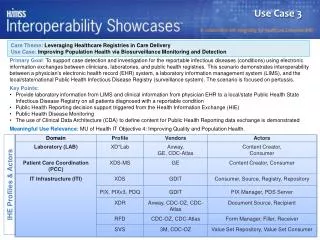
Current Data Warehouses REGION 2 REGION 1 REGION 4 V20 V19 V21 Guam V22 V18 Philippines CDW REGION 3 Alaska Hawaii Puerto Rico 2
VA Data Warehouse • All Available Results (since1996): • Patient Demographics • Outpatient Prescriptions • Visits • Discharges • Lab results • Problem List/Diagnoses • Vital Signs
Population Management Tools • Disease registries • Stratification by risk, severity, complexity, or need • Triage to appropriate provider • Cohort tracking: follows progress of patient cluster • Visit management: prepares patients for appointment • Prevention management: performs tasks on behalf of PCP • Consult management • Prioritizing referrals • Identifying missed cases • Medication management: prescribing patterns, safety, cost, adherence, poly-pharmacy • Resource management: systematic review of demand for services and rational resource allocation • Geographical information systems: track patient movements
Not Another Dashboard Practitioner Patient Raw Data Data Warehouse
Not Another Dashboard System Analytics Practitioner Patient Stratification By Need Resource Allocation Tools Identifying Actionable Findings Automated Preventive Services Raw Data Application of Practice Guidelines Cohort Tracking To Resolution Robust Statistical Analysis Automatic Case Triage Data Warehouse Synthesized Clinical Variables Execution of Clinical Algorithms
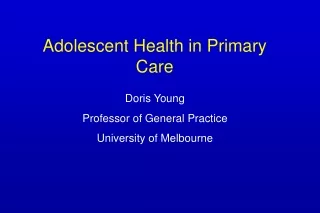
No Get A1c A1c Done? Decision Algorithm Yes No At Goal A1c >=7.0? Yes No Yes Evaluated Seen By PCP? On Meds? No Make Appt Yes No A1c Done? Get A1c Yes No A1c ≥ 9.0%? At Goal Yes No A1c ≥ 70 Days After Med Δ? Repeat A1c Yes Yes A1c Decreasing? Improving No Yes Seen by PCP? Evaluated No Take Action
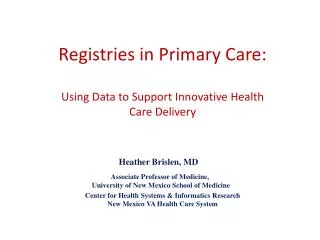
Chronic Elevation? Comprehensive Re-assessment Yes Glucose Profiling Sub-maximal Single OHA? RN No No Yes Glucose Profiling Maximal Single OHA? No PCP On Insulin? No Glucose Profiling Yes Sub-maximal Double OHA? RN No Yes Maximal Double OHA? Glucose Profiling Yes PCP Glucose Profiling Yes Yes RN Triage On Basal? Glargine? No Glucose Profiling PCP or PharmD Yes On Regular? Glucose Profiling Yes CDE On RAI?
Design of VISN 18 Systems • Fully automated • Near real-time data acquisition (e.g. within hours) • Highly sensitive case identification • Rigorous assessment of health status • Every patient • Every day • Using all relevant source files • Going back as far as possible • Data assembly across entire system • Derivation of complex clinical parameters • Dates of onset • Diagnostic criteria scores • Temporal trends and trajectories • Cumulative disease burden • Dose equivalents
Design of VISN 18 Systems • Real-time monitoring of patient status • Aggregate drug dose • Poly-pharmacy • Medication adherence • Appropriate drug dosing • Drug interaction monitoring • Drug contraindication monitoring • Robust statistical treatment of the data • Time-weighted averaging • Data transformations • Outlier identification (z-scores) • Drug dosing • Outcomes • Cost • Retrieval or synthesis of covariates
Design of VISN 18 Systems • Automatic application of practice guidelines • Change in patient status relative to current guidelines • Rapid dissemination of new recommendations • Execution of decision algorithms and clinical pathways • Analytics that replicate clinician’s decision process • Algorithm categorizes patients into groups for which a common action is indicated • Each group represents unique “covariate pattern” in data • Determining whether items are “actionable” • Event mapping: tests, visits, and treatment changes • Determines whether actions are indicated or already taken
Design of VISN 18 Systems • Stratification: • By risk for aggressive preventive measures • By severity for treatment intensification • By complexity for care coordination • By need often due to health literacy or social barriers • At any time, treatment directed at patients most likely to benefit until resources exhausted • Triage to appropriate team members • Based upon pre-determined roles • Assures that each team member practices at highest skill level
Design of VISN 18 Systems • Cohort tracking to problem resolution • Consult generation • Appointment scheduling • Outpatient visit • Diagnostic procedure or treatment • Other utilities • Failure analysis: determines relationship between causal factors and outcomes • Comparative effectiveness: compares alternative treatments • Practice profiling: variances and “best practices” • Research